Dupuytren’s disease is shortening and thickening of the palmar fascia on the affected digit(s). These flexion contractures generally develop slowly and are permanent and irreversible. More men than women are affected by this condition. Of note, 20% of people with diabetes will go on to develop Dupuytren's disease. Often diabetics will be more severely affected by this disease.
Diagnosis
History and physical examination: patients present with nodules, indentations or cords that develop under the skin in the palm of the hand, slowly developing a flexion contracture of the affected digit(s).
Signs and symptoms
Mild - Moderate
Palmar nodules
Palmar pits
Mild - no contracture PIP, MCPJ <30 o
Moderate – contracture PIP <30o, MCPJ 30-60o
+/- pain (may be pain at initial onset or during an active stage)
Moderate - Severe
Contracture
1st Web
MCPJ >60o with reduction in ADL
PIPJ >30o with reduction in ADLs
Recurrence / extension
Diathesis
Garrod's Pads
Differential diagnosis
Severe trigger finger
Flexor tendon/sheath tumour
Recent trauma, tendon rupture
Clinical testing
Physical Examination
Examination should include determination of the extent of the disease, skin involvement and measurement of any joint contractures.
Hueston’s Tabletop Test: a positive test is when a patient is unable to place all fingers in a flat position on a tabletop.
Management (mild to moderate symptoms)
Reassure the patient and give information on Dupuytren’s disease:
NHSGGC Hand Service Orthopaedics and Therapy Post Operative Guidelines: Dupuytren’s Contracture - Fasciectomy
Day of Surgery
Record pre-operative contracture
Operative procedure recorded, including any contracture that was not correctable
Hand placed in padded bandage/ slab and elevated as per surgeons protocol
Check circulation, sensation and movement (CSM)
Patient provided with post operative patient information sheet if they do not already have one
Fit note provided for the duration of expected absence if required
Arrange an urgent appointment with hand therapist in addition to nurse led dressing clinic appointment if required per surgeon’s protocol.
First Review Clinic (3 - 7 days)
Reduce dressing
Clean and check wound site (leave sutures in situ)
Any evidence of infection contact surgical team
Redress wound and apply light dressing
Advise on active/ passive ROM exercises as per patient information leaflet 4-6 times per day
The patient may be provided with a splint depending on surgeon’s protocol
Re-assure the patient that if the wound bleeds this is ok
If wound dressing becomes exceptionally soiled before next appt, patient can contact clinic
Arrange follow up appointment for 1/52 at review clinic
Provide post operative patient information leaflet if the patient does not already have one
Subsequent Review Clinic
Sutures removed at 10-14 days post op
Check CSM and assess for wound infection/ breakdown as above
Once wound has healed gently massage with an emollient hand cream 3-4 times daily
Check fitting of splint (if they have a splint)
Over subsequent visits the aim is to have a healed wound, full composite flexion and maintenance of the extension obtained on the operating table (Please refer to op note)
Monitor as required until wound healed and/or until therapy no longer required
Further review if required, depending on clinical progress
NHSGGC Post Operative Guidance for Therapy Intervention: Fasciectomy for the correction of Dupuytren’s
This information is intended for use with all patients with a diagnosis of Dupuytren’s disease who have undergone corrective surgery.
A large number of these patients require minimal intervention. To ensure effective and efficient management the clinician should have knowledge of:
How to actively and passively mobilise
The frequency of exercise
The period of time they should continue to mobilise and stretch
Functional outcome measures such as the DASH or quick DASH can be used to record functional outcome if desired.
First Appointment
5 step check list:
ROM – check ROM which was attained on operating table (op note). Record current ROM
Review and/or introduce exercises
Education and reinforcement of advice
+/- provision of thermoplastic splint (unit specific)
Agree plan for future intervention
1. ROM
Active Flexion – to flex all digits towards the distal palmar crease
Active Extension - to extend the digits till the end of a pain free range of movement and maintain/ achieve correction obtained on the operating table
Check wrist movement
Check thumb movement
Finger abduction and adduction
2. Exercise
Refer to exercises in the patient information leaflet (reference number to be added once confirmed by medical illustrations). Additional exercises or modified exercises can be issued as determined by assessment and clinical need.
Regularity of exercises to be at therapist discretion, taking into consideration any post surgery inflammation and oedema. Aim for exercises to be done 4-6 times per day.
3. Education
Aims:
Promote good hand hygiene
Prevent/minimise infection
Manage/limit oedema
Promote good scar management
Recover function
Hand Care
Hygiene:
Patient to wipe non affected areas with non-perfumed wipes.
Dressing should be kept clean and not soaked in water until stitches have been removed and the wound is well healed. Once the wound is healed patient can be advised to shower. Until then, if they need to shower, a plastic bag should be placed over the hand to keep the wound dry.
Oedema management:
Patient is advised to position the forearm in elevation using pillows when sitting/ sleeping.
Patient is advised to maintain range of movement of wrist, elbow and shoulder regularly.
Scar management and monitoring for signs of infection:
Once the wound is healed massage of the scar with a non perfumed emollient should begin. Patients should be taught to use circular motions along the scar working distal to proximal to help reduction of oedema. Evidence suggests that STM massage of the wound region reduces the thickening of the new scar tissue.
If there is any concern regarding the possibility of infection e.g. foul smell, oozing wound, redness, temperature, increased pain, this must be checked ASAP with a more experienced member of staff, the dressing clinic, a medic or practice nurse.
Function
Patient should be advised to move and use the arm and hand as pain allows. Remember for the first couple of weeks they should avoid heavy lifting/pulling.
Driving
Patient can return to driving as soon as pain allows and they feel that they are in complete control of the car. Advise that it is their responsibility to check with their insurance company before returning to driving.
Return to work
Time off work will depend on the patients occupation and, or place of work. We advise that you avoid all heavy lifting for at least 6 weeks.
4. Thermoplastic splints
Splinting is not routinely used in GGC and is only advocated by certain surgeons, please check local protocol before considering.
If you have any splinting questions or concerns please contact your local hand therapist (refer to details at bottom of page).
Splinting, if advocated, can be introduced at night to provide a low tension stretch. Extreme Tension should be avoided to prevent wound healing problems (dehiscence/ increase local inflammation).
If the patient has been issued or advised to wear a splint at night, please note that they should continue to do so for a period of up to 3 months. Please check with your local hand therapist if you are unsure what the operating surgeon advises. Patients should to be advised to report any problems or pressure areas with the splint as and when they arise. A small piece of tubi net can be issued to wear under the splint to assist with comfort and to absorb perspiration.
All the above advice and exercise is re-iterated and exercises progressed or modified as determined by clinical need and as pain allows.
ROM progression
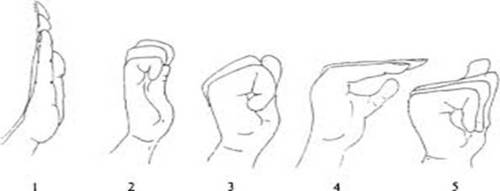
As well as practising composite flexion, attention may be required to hook grip, individual MCPJ, PIPJ and DIPJ flexion / extension. This can become easier for the patient as the wound heals, the stitches are removed and the swelling subsides. Nerve tendon gliding exercises are a useful adjunct exercise in addition to the basic exercises given to help achieve this.
The patient is taught and shown how to move through positions 1-5, and advised to repeat the sequence 10 times. This is repeated x 4 a day.
From: Akalin, Elif, et al. Treatment of Carpal Tunnel Syndrome with Nerve and Tendon Gliding Exercises. American Journal of Physical Medicine & Rehabilitation, vol. 81, no. 2, February 2002, pp. 108-113.
Summary
Targetable ROM is that which was achieved on the operating table.
Every patient is different. Some will require minimal intervention, others will require more. Assess and arrange for ongoing therapy, as necessary following local physiotherapy referral protocols.
The importance of wound care and scar massage cannot be underestimated. Evidence suggests that STM massage of the wound region reduces the thickening of the new scar tissue.
Some patients will inevitable encounter unexpected complications. If in doubt or any concerns please contact your local hand therapist.
Problematic Pain
Consult the Pain Service for information and guidelines on diagnosis and management of Complex Regional Pain Syndrome.
Huisstede BMA, Hoogvliet P, Coert JH, Fridén J; European HANDGUIDE Group. Dupuytren disease: European hand surgeons, hand therapists, and physical medicine and rehabilitation physicians agree on a multidisciplinary treatment guideline: results from the HANDGUIDE study.Plast Reconstr Surg. 2013;132(6):964e-976e. doi:10.1097/01.prs.0000434410.40217.23
 GGC - MSK Index
GGC - MSK Index