 Vascular surgery
Vascular surgery

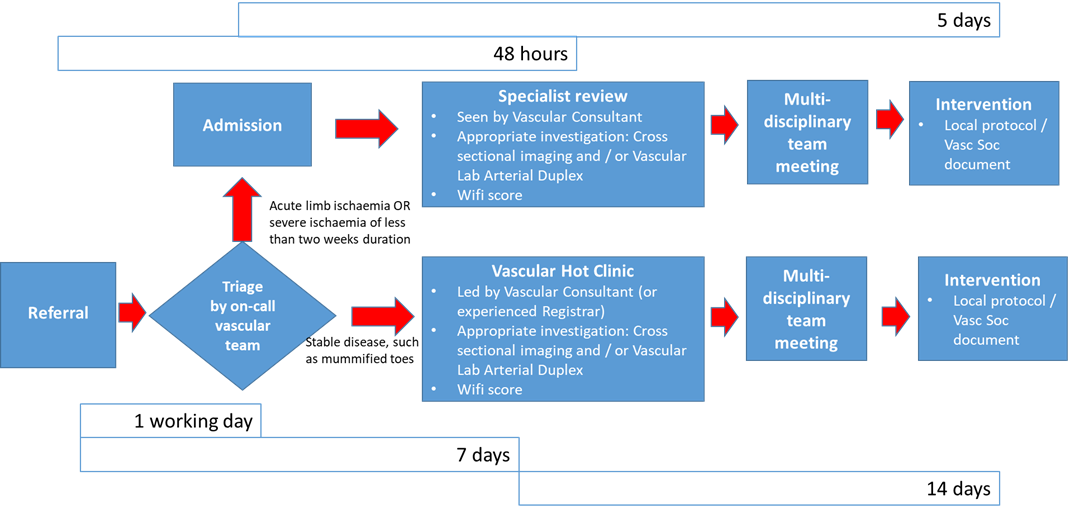
This document outlines a national model for the assessment and management of Chronic Limb Threatening Ischaemia (CLTI). It is closely based on the relevant section of the Vascular Society document A Best Practice Clinical Care Pathway for Peripheral Arterial Disease.
The principle of timely access to expert Vascular opinion with appropriate diagnostics and intervention is key to offering a safe and effective pathway for the management of patients with limb threatening ischaemia.
The Vascular GIRFT report highlighted that the delivery of revascularisation for CLTI across the UK was variable, with unacceptable delays in management pathways and this has led to significant differences in length of hospital stay and patient outcomes.
As set out in the Vascular Society document A Best Practice Clinical Care Pathway for Peripheral Arterial Disease, evidence-based management involves early and appropriate revascularisation to prevent limb loss; delay is best avoided by well organised networks with clear referral pathways.
Assessment of patients requires a multi-professional team, the lower limb Multi-Disciplinary Team, available 24/7. In order to deliver such care an adequate workforce with timely access to the appropriate facilities needs to be in place.
Chronic Limb Threatening Ischaemia definition:
Chronic Limb Threatening Ischaemia is the advanced stage of Peripheral Arterial Disease (PAD) where the blood supply to the foot is insufficient for the needs of the tissues. Without adequate treatment there is a significant risk of major limb loss.
persistently recurring rest pain requiring analgesia for more than 2 weeks
OR
ulceration
OR
gangrene of the foot or toes
AND
ankle pressure < 50mmHg
AND / OR
toe pressure <30mmHg
 Scan the code to visit our website
Scan the code to visit our website