 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland
- obesity
- increasing age
- male
- alcohol
- sedatives
- certain craniofacial characteristics
- retrognathia
- enlarged tonsils
- macroglossia
Sleep apnoea (Guidelines)

Warning
Objectives
Author is aware that this guidance is due for review and plans to review this by 28/02/2026.
The guidance can continue to be used in this interim period.
If you have any queries, please contact the guideline author/reviewer.
Obstructive Sleep Apnoea Syndrome (OSAS) is a common condition affecting all age groups.
In the middle aged population it affects 2-4% of men presenting a significant public health concern due to the associated cardinal daytime symptom of excessive sleepiness.
During sleep there is a loss of stability of the upper airwaywhich leads to pertial closure (hypopnoea) or complete obstruction (apnoea). This is associated with a drop in oxygen saturation and is terminated by a large inspiratory breath and arousal from sleep. The patient is often unaware of these events however their bed partners are often able to provide witnessed accounts of apnoea, chocking episodes and heroic snoring.
Although the breathing distrubance occurs during sleep the consequences of the fragmented sleep affects daytime functioning.
Excessive sleepiness impairs quality of life affecting relationships and cognitive function.
It also affects work performance and people with untreated apnoea are seven times more likely to have an RTA (NICE 2008), which may be due to a lapse in concentration, error of judgement or falling asleep at the wheel.
OSAS is also associated with hypertension which increases the risk of cardiovascular disease and stroke. (IMPRESS 2009) Although it is strongly connected with obesity, 30% of patients have a BMI <30.
- excessive sleepiness which can affect cognitive function, mood and quality of life
- morning headaches
- waken non refreshed
- poor concentration / ability to make decisions
- impaired work performance
- difficulty driving - concentration lapse can be fatal
- reduced libido
- personality change- irritability, anxiety, aggression, depression
- snoring
- apnoea
- choking episodes
- waken gasping
- frequent wakenings
- restless sleep
- fragmented sleep
- sleep deprivation
- idiopathic hypersomnolence
- shift work
- depression
- narcolepsy
- hypothyroidism
- RLS/PLM
- medication
- sedatives
- caffeine
- theophylline's
- amphetamines
- beta blockers
- SSRI
- excess alcohol
- neurological conditions
- dystrophica myotonica
- previous head injury
- Parkinson's
Medication and alternative causes of sleepiness
- fragmented sleep
- sleep deprivation
- idiopathic hypersomnolence
- shift work
- depression
- narcolepsy
- hypothyroidism
- RLS/PLM
- medication
- sedatives
- caffeine
- theophylline's
- amphetamines
- beta blockers
- SSRI
- excess alcohol
- neurological conditions
- dystrophica myotonica
- previous head injury
- Parkinson's
If the following signs and syptoms present
- Epworth Sleepiness Score >11
- excessive daytime sleepiness which can affect cognitive function, mood and quality of life
- waken non refreshed
- snoring
- apnoea
- morning headaches
Refer via SCI Gateway
1. avoid sedatives
2. stop smoking
3. reduce alcohol intake and avoid alcohol 4 hours before bed
4. try to sleep on side
5. elevate bed head by 30 degrees
6. weight loss if BMI >25
7. encourage excercise
8. follow good sleep hygiene principles
9. if patient reports sleepiness while driving, advise they must stop until assessment complete
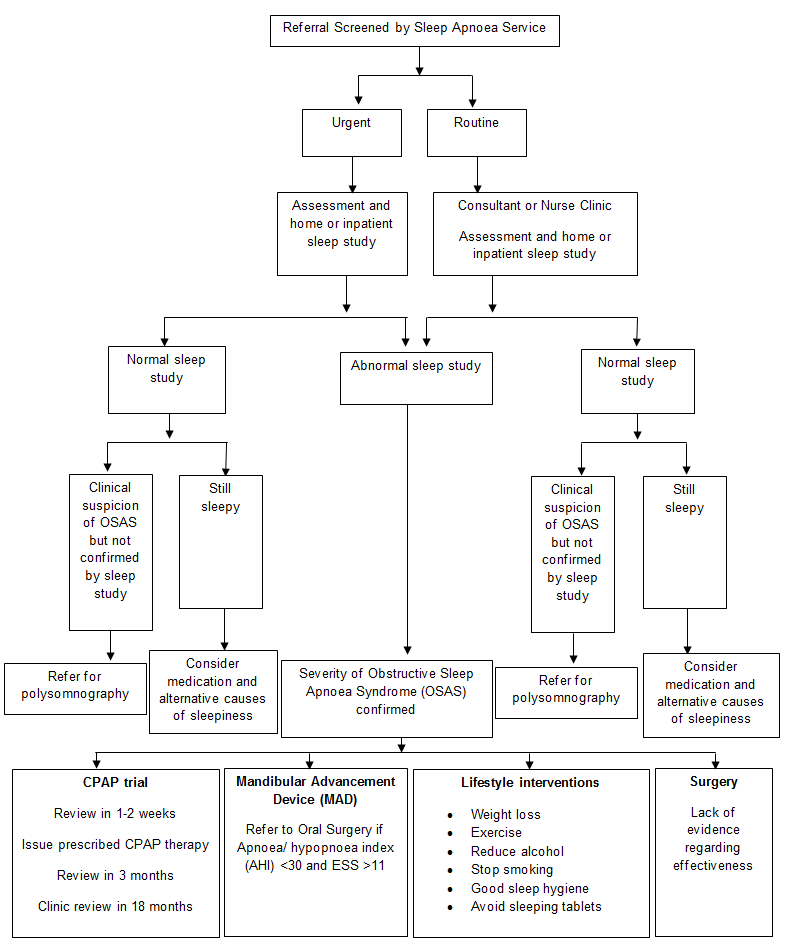
Classification of Obstructive Sleep Apnoea
DVLA - sleep apnoea
British Thoracic Society position statement: Sleep | British Thoracic Society | Better lung health for all
RLS: Restless Leg Syndrome
PLM: PLMPeriodic Limb Movements
SSRI: Selective serotonin reuptake inhibitors
BMI: Body Mass Index