Overreliance on SABA is an indicator of poor asthma control.20,26 It is essential that patients who appear to be overusing SABA inhalers are assessed for control of symptoms as part of a holistic asthma review. Asthma control test (ACT) questions highlight that a patient is not controlled if they use a SABA inhaler three or more times in a week.6 The National Review of Asthma Deaths (NRAD) report22 found that patients who used more than 12 reliever inhalers per year were at a greater risk of uncontrolled asthma and sudden death. There was evidence of under-prescribing of preventer medication. Use of 12 SABAs in one year implies the use of 46 puffs in one week and for six SABAs a year is 23 puffs a week.23 In the SABINA study,24 an association across all asthma severities was found between high SABA use, of more than three inhalers per year, and an increase in exacerbation rates and healthcare utilisation.25 It is crucial that patients understand the importance of when and how to use their inhalers and of adherence to therapy with their preventer inhaler.22
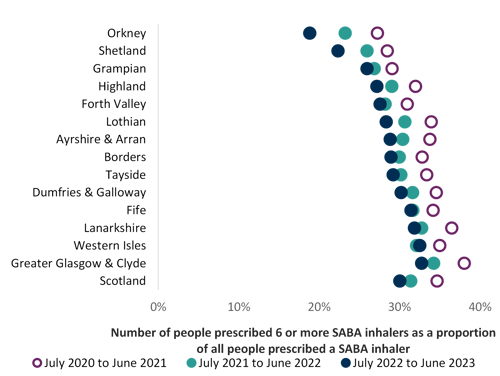
The main focus of an asthma review is to ensure that the individual’s condition is well controlled, they are prescribed the optimum inhaler therapy in alignment with current guidance and are using their inhalers effectively. We know that there are many people with asthma in Scotland who are prescribed six or more SABA inhalers in 12 months (see Chart 1 below). Use of three or more SABA inhalers is associated with a higher rate of exacerbations and hospitalisation.24
Following clinical consensus regarding asthma control, this indicator has been reduced from the previous 12 SABA inhalers prescribed annually to recommend that a patient prescribed six or more inhalers annually is a trigger for timely, priority review (see Chart 1). This should ideally take place before the issue of the next prescription. Review is required for those using three or more SABA inhalers, but prioritisation may be considered for those using six or more SABA inhalers.25
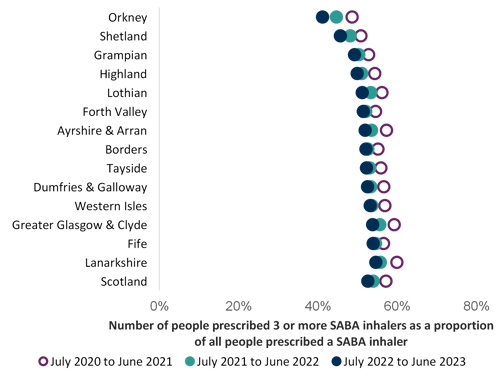
This guide includes an indicator chart of people prescribed three or more SABA inhalers as an aspirational level, as a person with well-controlled asthma would need no more than this (see Chart 2). This should be discussed at their annual routine review. This indicator is a guide and is unable to distinguish between people with asthma and COPD.
SABAs are not first step maintenance treatment for asthma, a low dose ICS is recommended.6 The Global Initiative for Asthma (GINA) guidelines recommend initiation of ICS-containing treatment when, or as soon as possible after a diagnosis of asthma is made.26 They recommend reliever therapy using an anti-inflammatory reliever (AIR), a low-dose combination ICS-formoterol inhaler taken as needed as preferred step one treatment.26 As-needed low-dose ICS-formoterol reduces the risk of severe exacerbations and emergency department visits or hospitalisations by 65% compared with SABA-only treatment.27 Licensed indications for products and local formularies should be checked for choice of low-dose ICS-formoterol combinations, where appropriate, if prescribing the AIR regimen.
It should be noted that emergency supplies of SABA inhalers are possible to obtain from the community pharmacy. Liaison with community pharmacy colleagues is advised to help reach those people with asthma who may be poorly controlled and do not attend asthma reviews.
The Scottish Therapeutic Utility (STU) software (chapter 12) is recommended, to support GP Practices to identify individuals with asthma who are over-reliant on SABA inhalers using practice coding.
 Respiratory: Quality prescribing strategy - a guide for improvement
Respiratory: Quality prescribing strategy - a guide for improvement