SIGN 158 recommends the following for adults and children.6
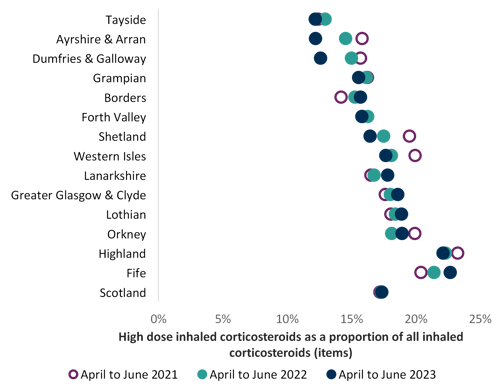
Patients should be maintained at the lowest possible dose of inhaled corticosteroid. Reduction in inhaled corticosteroid dose should be slow as patients deteriorate at different rates. Reductions should be considered every three months, decreasing the dose by approximately 25 to 50% each time. It is difficult to set a specific threshold level of ICS inhalers for review due to their varying potencies, dosing and quantities (for example 200 actuations in most ICS MDIs and 100 doses in some ICS DPIs).
It is important to arrange for a regular review of patients as treatment is reduced. When deciding the rate of reduction, it is important to take into account the following aspects: the severity of asthma, the side effects of the treatment, time on current dose, the beneficial effect achieved, and patient preference.
The dose – response curve for inhaled corticosteroids (below)32 shows the difference in clinical effect and side effects when a corticosteroid dose is increased. At doses of 800 micrograms per day and above, the clinical benefit of increasing inhaled corticosteroid dose is outweighed by increase in side effects.
Dose–response curve for inhaled corticosteroids
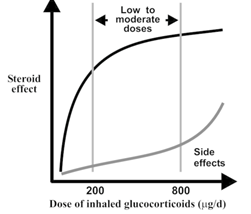
Reproduced with permission from National Library of Medicine (Hannu Kankaanranta, Aarne Lahdensuo, Eeva Moilanen, and Peter J Barnes)32
 Respiratory: Quality prescribing strategy - a guide for improvement
Respiratory: Quality prescribing strategy - a guide for improvement