The Trauma Team Leader will complete the pre-arrival checklist below.
TTL pre-arrival checklist - adult trauma
Staff
|
Time/tick
|
| Trauma call 2222 |
Adult code red trauma call ARI Resus |
|
| Adult Trauma call ARI Resus |
|
| Other Specialties Consider if multiple pts. |
Plastics 4316 |
|
| Neurosurgery 2334 |
|
| Cardiothoracic 2799 |
|
| Assign medical roles |
|
|
| Assign nursing roles |
|
|
| Assign Scribe |
|
| Don appropriate PPE, Apply Role label and print name on PPE |
|
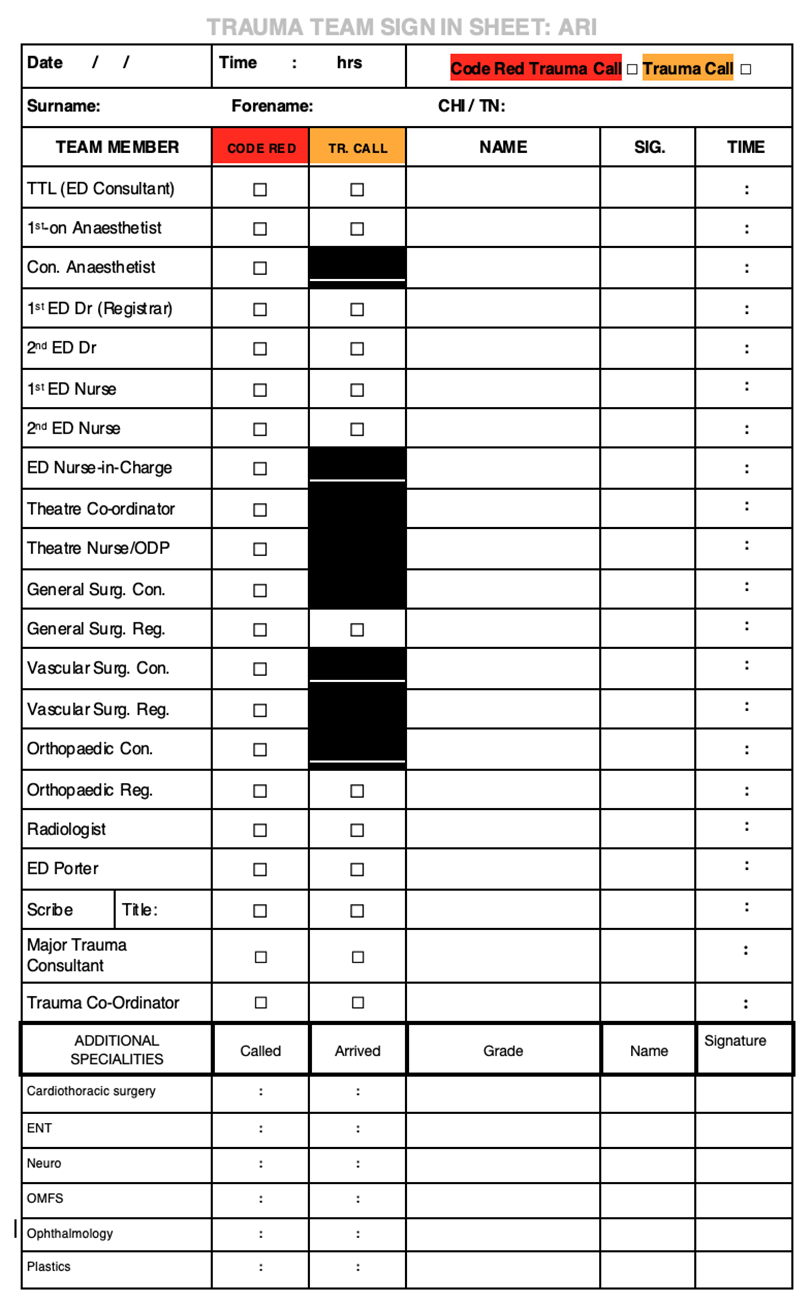
| Ensure staff sign in |
|
Blood
|
| Code Red Protocol – activated when called by prehospital team |
|
| Major Haemorrhage protocol – activated when patient arrived |
|
| Extreme circumstances – unable to wait for SNBTS sample – request “Bulk shipment of Emergency blood” |
|
Equipment – Trauma cabinet
|
| Disrobe |
Trauma shears |
|
| On bed/ ambient |
Trauma mattress |
|
| Blue bed cover placed over trauma mattress |
|
| Bair hugger under body |
|
| Pelvic binder on bed |
|
| Turn up ceiling radiant heater |
|
| A |
Airway trolley with kitdump performed |
|
| Check Video laryngoscope – battery |
|
| Suction check |
|
| B |
NRB mask O2 attached and at 15 litres |
|
| BVM to hand – O2 attached 15 litres |
|
| Ventilator – checked and on standby |
|
| C |
Level one/Blood warmer – on and run with saline |
|
| Cannulation kit - blood tubes – pink, purple, blue, green. |
|
| Appropriately sized IO needle and drill battery check |
|
| Ultrasound switched on and gel |
|
| Trauma chest drain – Unisurge kit |
|
| Thomas splint/CAT tourniquet |
|
Drugs
|
| RSI drugs See RSI drug drawing guide |
Fentanyl – 500mcg in 10mls |
|
| Ketamine – 200mg in 20mls |
|
| Rocuronium – 100mg in 10mls |
|
| Metaraminol – 10mg in 20mls |
|
| Ephedrine – 30mg in 10mls mg in 10mls |
|
| Propofol Infusion |
|
| Consider metaraminol infusion |
|
| Others |
TXA – within 3 hours of injury – clinical concern ongoing haemorrhage Bolus 1g given over 10 minutes Infusion – 1g in 500mls saline - 8 hours (62.5mls/hr.) |
|
| Analgesia |
IV Paracetamol 1g in 100mls (body weight >50kg) |
|
| IV Morphine 10mg in 10mls |
|
| Antibiotics for open fracture Asap, aim for <3 hrs from injury for KPI |
Co-amoxiclav 1.2g |
|
| Clindamycin 600mg IV - If penicillin allergic |
|
Others
|
| Add details to the ATMIST board |
|
| Pre book patient on TRAK – call reception 53306/50506 |
|
| Book as unknown patient if unable to confirm details |
|
| Request trauma CT |
|
| Request bloods |
|
| Ensure correct trauma documentation |
|
| Add major trauma consultation – bone icon |
|
Perform Team brief
|
STAND DOWN CODE RED once appropriate. Return & preserve blood products as able.
 North of Scotland major trauma guidelines
North of Scotland major trauma guidelines