 NHSL Referral Pathways
NHSL Referral Pathways
- Chronic widespread pain (3 or more months of generalised pain, affecting both sides of the body and above and below the waist, with no other explanation)
- Widespread tenderness
- Fatigue
- Non-refreshed sleep
- Mood disturbance
- Cognitive impairment
Fibromyalgia Referral Guideline
Warning
Fibromyalgia (FMS) is a syndrome of chronic widespread pain and tenderness associated with fatigue, unrefreshing sleep and perception of cognitive dysfunction. There is no organic muscle or joint pathology.
Diagnosis of the condition should be primarily conducted in primary care however a secondary care referral should occur when there is diagnostic uncertainty.
Widespread tenderness.
Previous diagnostic criteria for fibromyalgia have included specific tender points on examination but these have proved hard to standardise and are not required for diagnosis.
Fibromyalgia is a clinical diagnosis. There are no specific diagnostic tests. Simple blood tests are normal although FMS can coexist with other diseases.
- U&E, LFT, TFT, bone profile
- ESR and CRP
- Information such as: Fibromyalgia by Versus Arthritis and Fibromyalgia by Michigan Medicine (University of Michigan)
- Regular aerobic exercise (20 minutes 2-3 times per week).
- A pain management approach including elements of education, exercise and psychological support such as CBT. Please refer to:
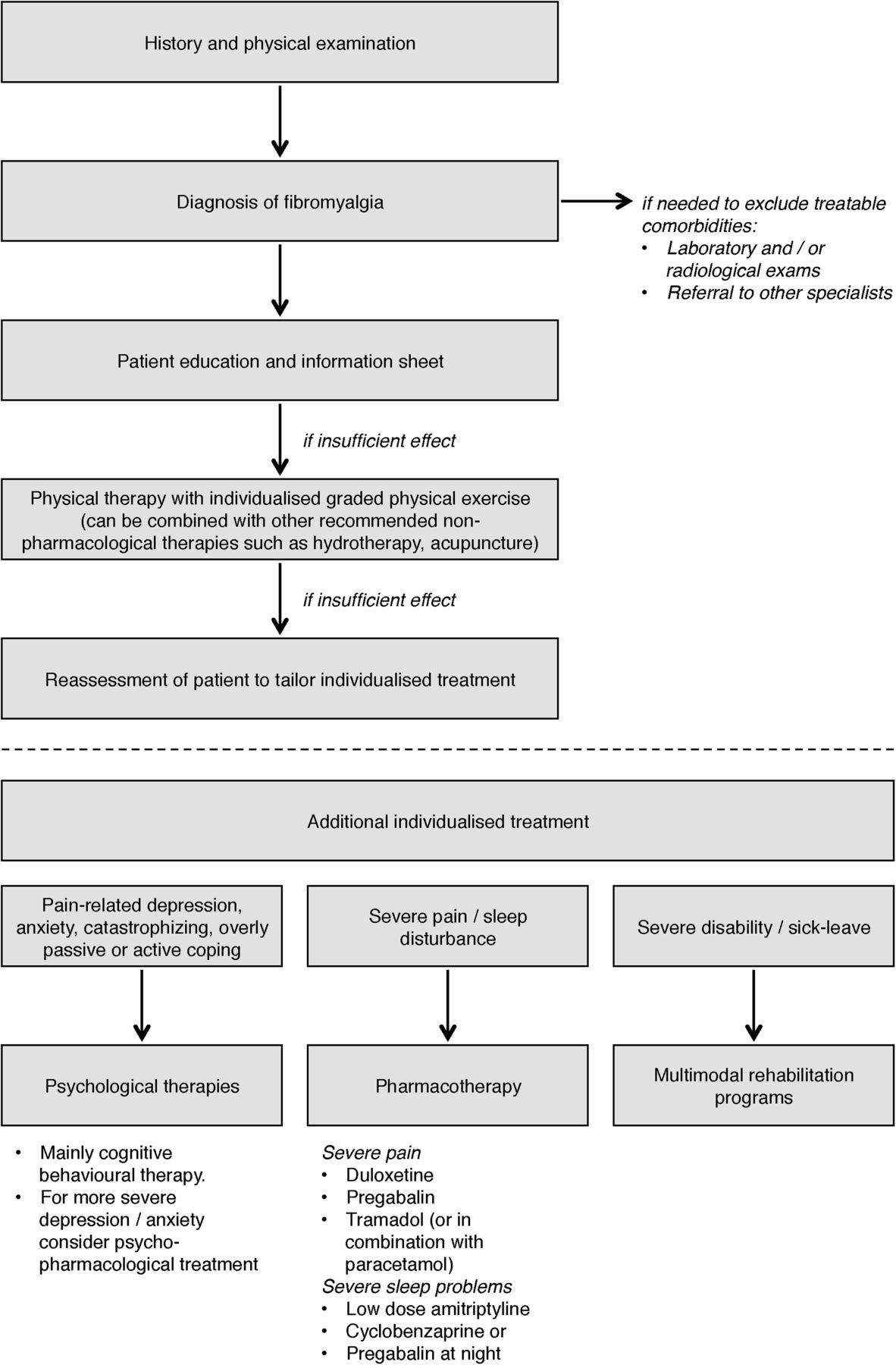
- Management recommendations as flow chart (Macfarlane G.J., Kronisch C., Dean L.E., et al (2017) 'EULAR revised recommendations for the management of fibromyalgia', Annals of the Rheumatic Diseases, 76(2), pp. 318-328. Available at: https://ard.bmj.com/content/76/2/318. (Accessed: 8 September 2021).
- Fibromyalgia: Tools by Michigan Medicine (University of Michigan).
- Management recommendations as flow chart (Macfarlane G.J., Kronisch C., Dean L.E., et al (2017) 'EULAR revised recommendations for the management of fibromyalgia', Annals of the Rheumatic Diseases, 76(2), pp. 318-328. Available at: https://ard.bmj.com/content/76/2/318. (Accessed: 8 September 2021).
- Many reviews have indicated that antidepressants are useful in the treatment of fibromyalgia; the best evidence for improvement in pain and in quality of life is for duloxetine and for pregabalin (neither is licensed for the treatment of fibromyalgia in the UK).
- Patients with joint swelling and tenderness.
- Patients with joint pain and elevated inflammatory markers (ESR and CRP).
- Patients in whom there is clinical suspicion of underlying connective tissue disease – patients with a photosensitive rash, Raynaud’s, recurrent oral ulceration or sicca symptoms and a positive ANA. A weakly positive (1:40 or 1:160) antinuclear antibody (ANA) is a common laboratory finding (seen in up to 15% of healthy people) and unless there are clinical features to suggest a connective tissue disorder, these patients will not require Rheumatology review.
- Patients with generalized pain and/or fatigue with no other symptoms or signs and with normal simple test results.
- Patients who have previously been discharged from Rheumatology with a diagnosis of fibromyalgia/widespread pain are very unlikely to benefit from further review and the process may simply delay referral to the Pain service.