Self care
The patient should be taught and encouraged to become independent with all aspects of laryngectomy and stoma care at the earliest opportunity post-operatively and education should be ongoing3. This process should be integrated into the patient’s normal activities of daily living.
Psychological impact of the laryngectomy
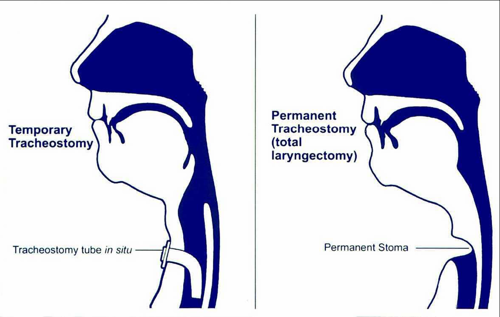
Laryngectomy results in loss of ‘normal’ voice and formation of a stoma. These changes mark the individual as different and some stigma may be attached to the changes causing negative reactions in others9. Perceived stigma can have a significant impact on work, recreation, financial situation, family relationships, social relationships, community involvement and self-expression and result in low mood and depression. Nurses can plan care strategies to minimise perceived and actual stigmatization and promote adjustment to the laryngectomy by the patient and their carers/family9.
Discharge planning
The discharge planning of any patient should commence prior to or on admission to hospital of a patient undergoing major head and neck surgery. Visiting the patient at home, prior to surgery would permit the community nurse to commence an assessment of the patient’s needs and social situation while the communication difficulties are limited. This may identify any potential issues or problems.
Discharge planning meetings should be encouraged, as this facilitates a multi professional approach to discharge and enables a seamless continuation of care.
If any relevant equipment is required to promote the discharge this will be the ideal opportunity for the community nurse to assess and plan for discharge. Within Ayrshire and Arran equipment is readily available for rapid delivery.
Once home the community nurse should be able to visit (if previously unable to) to asses both patient and home circumstances and any difficulties would be addressed. Community nurses work very closely with Social Services Departments and are able to liaise with colleagues to support patients at home. During this initial visit the community nurse would be aware of the patient’s level of independence with stoma care and of their present speech ability at this time. The community nurse would also be able to prescribe and or order any supplies the patient requires to continue with their stoma care. Community nurses will also be able to liaise with GP and community pharmacist with regards to medications required.
The nurse and the patient should be able to agree time and dates for further support contact. At this point the community nurse would give the patient the contact telephone numbers for the both the community nurses base and the out of hours contact details.
Training and education
Community nursing staff are encouraged to attend ENT ward to go over care prior to discharge of a patient with a laryngectomy. Alternatively, a joint visit may be performed with the Macmillan Head and Neck Cancer Nurse Specialist following discharge.
Individual patient care can be discussed and advice can be obtained by contacting ENT ward, Specialist SLT, Macmillan Head and Neck Cancer Nurse Specialist or ENT Nurse Practitioner.
 NHS Ayrshire & Arran guidelines
NHS Ayrshire & Arran guidelines