DGRefHelp - NHS Dumfries & Galloway
DGRefHelp - NHS Dumfries & Galloway
Cough is very common, representing 20% of referrals to respiratory medicine, and 10% of the population at some point in life. It is very common to not find a cause for a chronic cough; a cough present for 6 months or more is very unlikely to resolve. Reassessment following a failure to respond to treatment is unlikely to result in a different outcome.
There are no additional treatments available for cough beyond those conditions detailed in this protocol. Referral to secondary care is very unlikely to add anything to management in the context of normal investigations and clinical examination.
Key considerations
Acute cough, lasting less than 8 weeks, is usually associated with acute bacterial or viral bronchitis, or other respiratory infections. A new or changed cough may be the presenting symptom of a respiratory condition, particularly lung cancer.
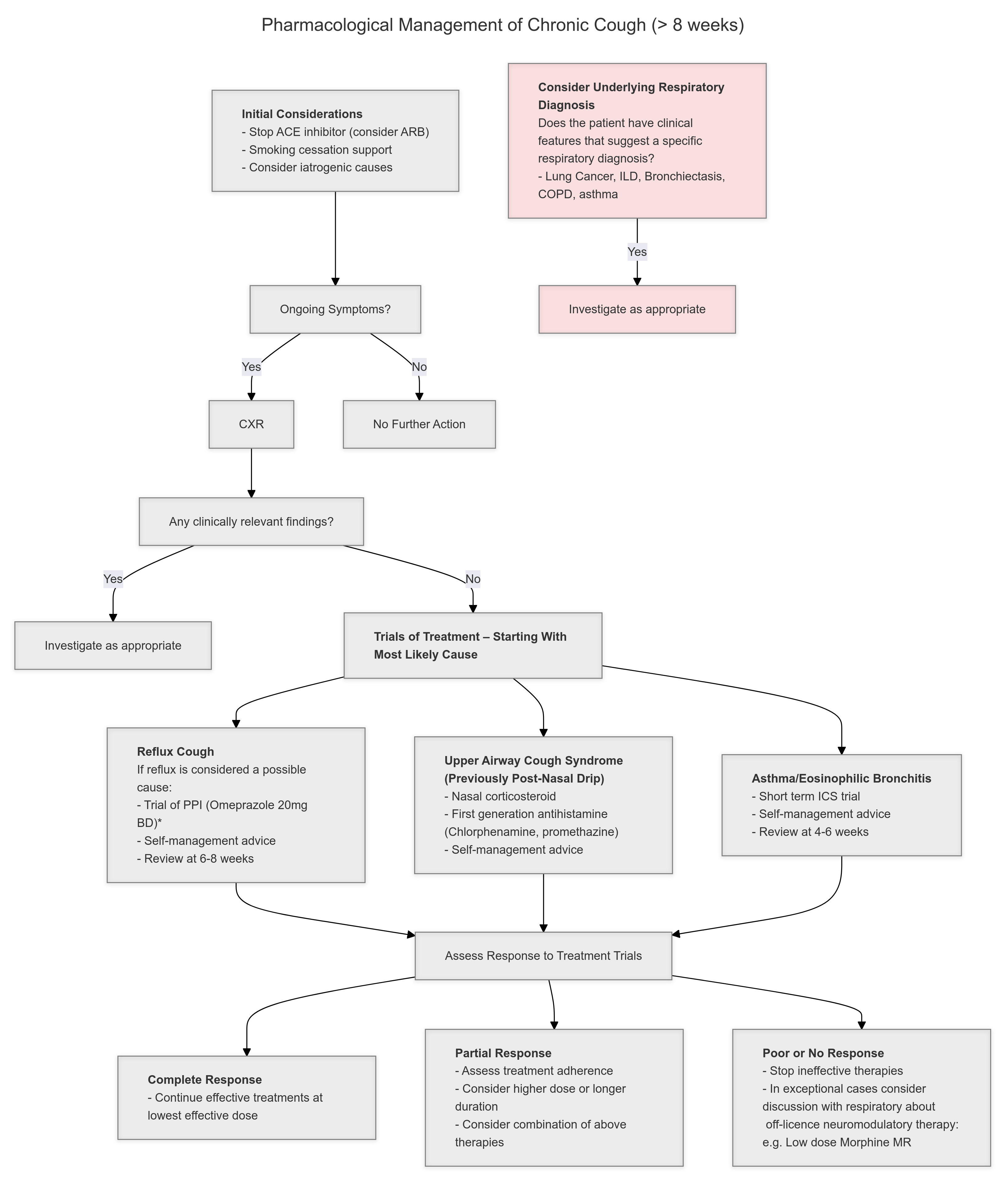
All patients with a new or changed cough must have a respiratory examination, and a CXR. An abnormal CXR should trigger consideration of CT scanning and discussion with secondary care.
Chronic cough is a cough lasting more than 8 weeks. The character of the cough is not helpful in differentiating the cause of the cough. Very common triggers for chronic cough are noxious stimuli (gastric fluid, smoke, particulates, hyper- or hypo-tonicity). A very common presentation is a chest infection that resolved with time, but the cough persisted long term, beyond the expectation for ‘post viral cough’.
It is common to elicit a history of attacks of coughing after:
- Laughing
- Talking on the telephone
- Moving from a warm environment to a cold environment, or vice versa
- Eating
- Coming into contact with strong smells (perfumes, flowers, food aromas)
The presence or absence of these features does not help in determining the likely aetiology.
A chronic cough is usually secondary to cough hypersensitivity, a heightened response to exposure to low levels of thermal, chemical or mechanical stimulation. The mechanisms of cough hypersensitivity are not fully understood.
Chronic Productive Cough should be investigated and managed considering the possibility of chronic bronchial infection, and bronchiectasis.