 Vascular surgery
Vascular surgery

An Abdominal Aortic Aneurysm (AAA) is a dilatation of the main artery in the abdomen which, once it reaches a certain size, may rupture and, without emergency treatment, this is likely to prove fatal. Ideally, AAAs should be detected prior to rupture so that they can be repaired surgically in a planned, elective manner.
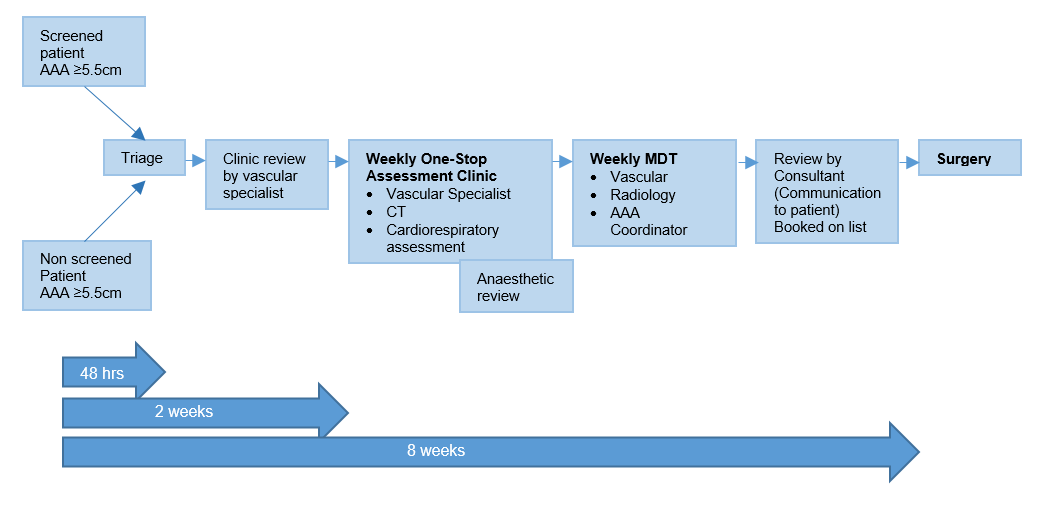
Abdominal Aortic Aneurysms (AAA) are currently identified by two different paths. The majority are found incidentally as a consequence of a scan for some other reason, the remainder by the National AAA Screening Programme, where men aged 65 are invited to participate in AAA abdominal ultrasound screening. Those found to have a large AAA (equal to or greater than 5.5cm in AP diameter) are referred urgently to Vascular Services. The AAA Screening Programme, via the Key performance Indicators, dictates that men who are found to have a large AAA are seen and treated within 8 weeks.
The Provision of Vascular Services 2021 document from the Vascular Society of Great Britain and Ireland states that all AAA above threshold, irrespective of how they were detected, should be treated in a similar manner with patients being seen within 2 weeks of diagnosis and being treated within 8 weeks. Previously, due to limited resources for assessment and intervention on AAA, screen-detected aneurysms may have been prioritised over those found incidentally. Currently those patients with an AAA discovered incidentally tend to wait longer for assessment and treatment compared to those with a screen-detected AAA leading to unacceptable inequality.
A single pathway should be established for all patients with aneurysms in Scotland, supported by a dedicated local co-ordinator, an efficient ‘one stop’ pre-operative assessment service, with ‘lifestyle’ advice given at the time of diagnosis, as well as adequate resource for timely operative intervention. For most patients it should be possible to complete this within 8 weeks of diagnosis.
 Scan the code to visit our website
Scan the code to visit our website