 Type 2 diabetes mellitus: Quality prescribing strategy - a guide for improvement
Type 2 diabetes mellitus: Quality prescribing strategy - a guide for improvement
Diet and lifestyle
- Type 2 Diabetes Mellitus (T2DM) treatment should focus on diet and lifestyle interventions at every stage of the person's journey, from newly diagnosed to complex care, as the need for increased medication can be reduced through weight reduction and dietary change.
- Prevention is better than treatment and so lifestyle and dietary interventions should be supported at all stages, both from a national policy perspective and individual support.
- Remission is possible through weight loss and dietary changes supported by local care pathways, including dietitians (see lifestyle interventions and remission).
Diabetes medicines
- If pharmacological treatment is needed, the risks and benefits of treatment should be discussed with the individual to enable shared decision-making, taking a person centred approach and using the 7-step review process. Continued effectiveness of treatment and targets should also be regularly reviewed.
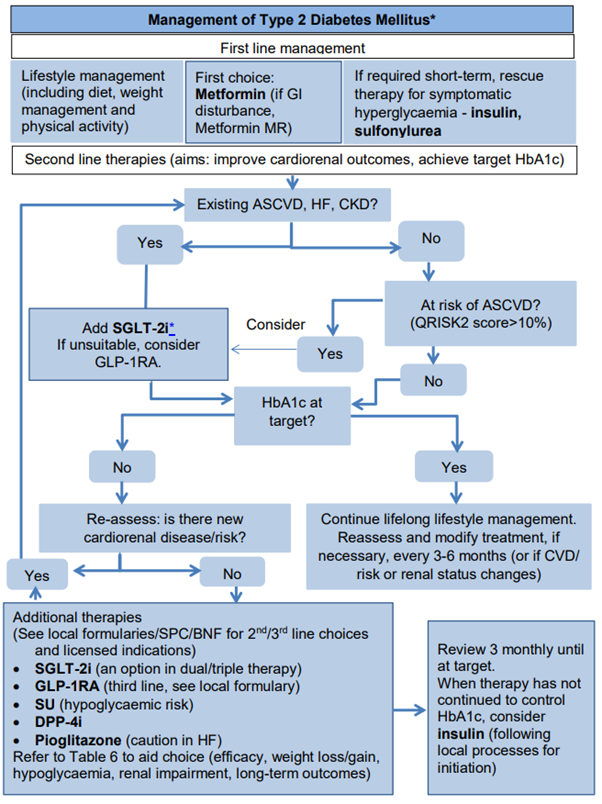
- Metformin remains the first choice for the pharmacological treatment of T2DM (unless contraindicated or not tolerated) (see metformin). This table provides a summary of medication characteristics for treatment T2DM.
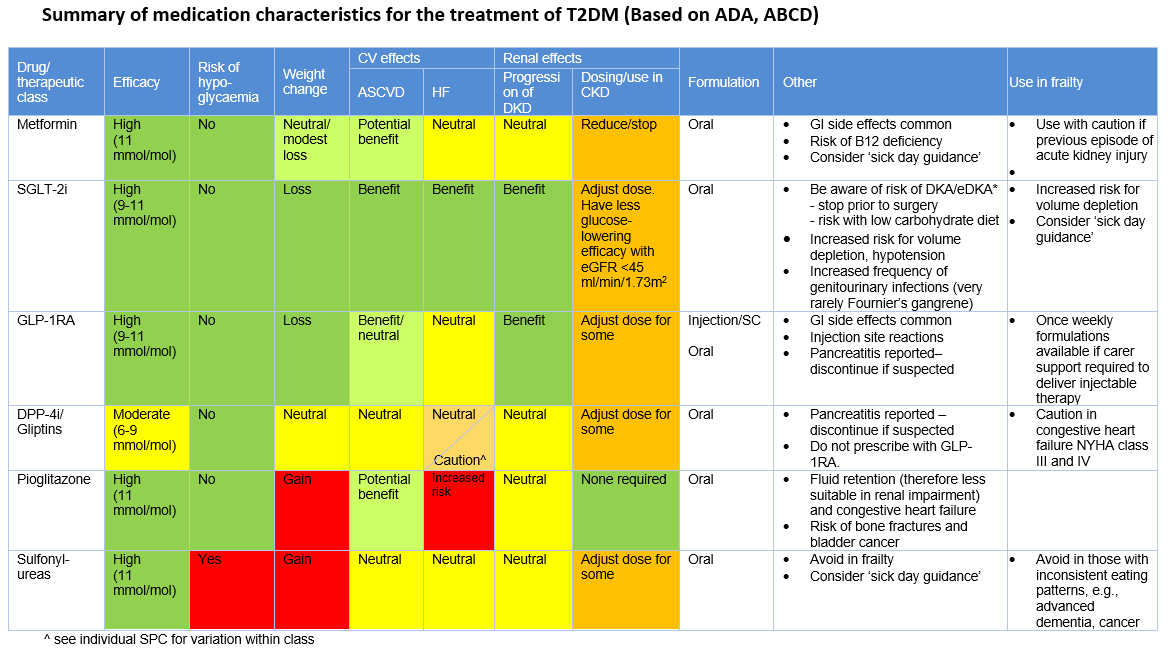
- Co-morbidities must be considered, especially atherosclerotic cardiovascular disease (ASCVD), heart failure (HF) and chronic kidney disease (CKD). Newer therapies [sodium-glucose co-transporter-2 inhibitor (SGLT-2i) and glucagon-like peptide 1 receptor agonist (GLP-1RA)] have positive outcomes for people with T2DM independent of glycaemic control (see cardiovascular and renal risk). See management of T2DM pathway for details of the treatment algorithm below, and prescribing choices for management of CKD.
- There is an increased incidence of euglycaemic diabetic ketoacidosis (eDKA) with SGLT-2i and additional advice is provided to support appropriate prescribing of these agents and minimise the risk of harm in their use.
- Insulin may be required by some people for treatment of T2DM, usually if other pharmacological therapy is no longer effective. (see 'insulin therapy').
- Polypharmacy is common in the treatment of T2DM. A polypharmacy review (following the 7-Steps approach) should ensure optimal management of T2DM and any other co-existing conditions. This should include addressing lifestyle factors and considering the most appropriate medication and dose for the individual, with regular reviews for continued effectiveness (see polypharmacy in diabetes).
- A person with T2DM should receive the appropriate treatment for their condition through regular reviews and shared decision making. Regular review of medicines and care outcomes guards against clinical inertia.
Blood glucose monitoring
- Self-monitoring of blood glucose is recommended for a limited group of people. Use of intermittently scanned or continuous glucose monitoring is increasing, and guidance continues to change to reflect this (see 'blood glucose monitoring').
Frailty and older adults
- For people living with frailty and for older people, the benefits of intensive treatment of T2DM should be balanced against the risk of potential hypoglycaemia and the consequences of falls, fractures and hospitalisation.
- Less stringent HbA1c targets may be appropriate for the frail and older person, in agreement with the individual (see frailty and older adults - for advice on managing T2DM in those with varying levels of frailty).
Mental health
- There is a higher incidence of depression and mental health problems in people with T2DM, which can lead to poorer outcomes for both conditions, and they should not be managed in isolation (see mental health).
- The prevalence of diabetes in 2020 was higher among those living in the most deprived quintile (10%) compared with those in the least deprived quintile (4%).
Environmental impact
- Healthcare and prescribing have an environmental impact, which should be minimised wherever possible (see 'polypharmacy in diabetes').