
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland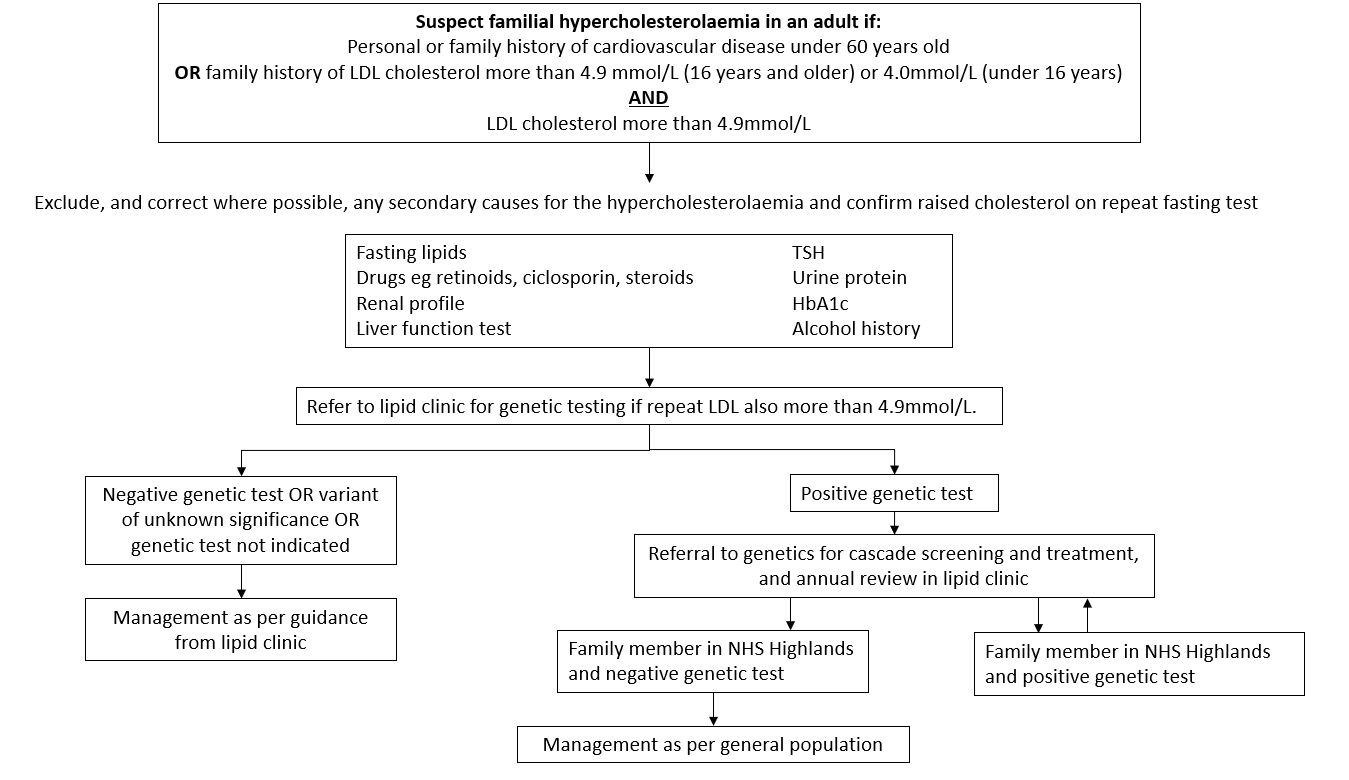
Diagnosing familial hypercholesterolaemia (guidelines)

Warning
What's new / Latest updates
New guidance
Diagnosing familial hypercholesterolaemia
Familial Hypercholesterolaemia is a monogenic disorder characterised by high concentrations of low-density lipoprotein (LDL) cholesterol. It is common with estimated prevalence around 1 in 350 people. Patients with untreated familial hypercholesterolaemia have an increased risk of premature cardiovascular disease; more than 50% in men and more than 30% in women are affected by 60 years.
This guideline is to inform primary and secondary care healthcare professionals when to consider familial hypercholesterolaemia, what investigations to do, where to refer to and likely outcomes.
All patient groups should be considered as to whether they meet these criteria.
For patients under 16 years old LDL cholesterol cutoff is 4.0 mmol/L. Paediatric familial hypercholesterolaemia is managed by centrally commissioned paediatric inherited metabolic medicine service. Contact lipid clinic for more details, if required.
If LDL cholesterol results are not available or triglyceride results are too high to allow calculation, use total cholesterol greater than 7.5 mmol/L (16 years or older) or 6.7 mmol/L (under 16 years).
Tendon xanthomas are rarely seen but if a patient has them or reports their relative does, and the patient’s LDL cholesterol is greater than 4.9 mmol/L, then they should be referred to the lipid clinic.
If family members are out with NHS Highland, the patient will be given letters to pass to their family members to allow local cascade testing for familial hypercholesterolaemia.
Patients who are relatives of known familial hypercholesterolaemia patients (and have not had cascade genetic testing for whatever reason) should not have the same criteria applied but should all be referred to the lipid clinic for consideration for genetic testing.
Familial hypercholesterolaemia causes a lifelong elevation of cholesterol, whatever the lifestyle, and hence the increased risk of cardiovascular disease eg. MI, CVA, PAD. If a patient has previously had lower cholesterol results (and was not on treatment at the time) it is unlikely to be familial hypercholesterolaemia and other causes for the newly raised cholesterol should be considered eg. hypothyroidism.
NICE Clinical Knowledge Summary on familial hypercholesterolaemia: https://cks.nice.org.uk/topics/hypercholesterolaemia-familial/
Familial hypercholesterolaemia: identification and management clinical guideline CG71: https://www.nice.org.uk/guidance/cg71
Heart UK: https://www.heartuk.org.uk/
British Heart Foundation https://www.bhf.org.uk/
| Abbreviation | Meaning |
|
LDL |
Low density lipoprotein |
|
MI |
Myocardial infarction |
|
PAD |
Peripheral arterial disease |
| TSH | Thyroid stimulating hormone |