IV ondansetron 0.15 mg/kg (maximum 4mg) should be given to children who have not already been given ondansetron for prophylaxis of POV
Ondansetron - There is no evidence demonstrating a benefit of timing ondansetron administration in children with respect to the time of surgery
- If required in patients under six months a dose of 0.1 mg/kg should be used
- Ondansetron and other 5HT3 antagonists should be avoided in children where prolonged QT interval is known or suspected
|
For children who have already been given ondansetron a second antiemetic from another class should be given, such as:
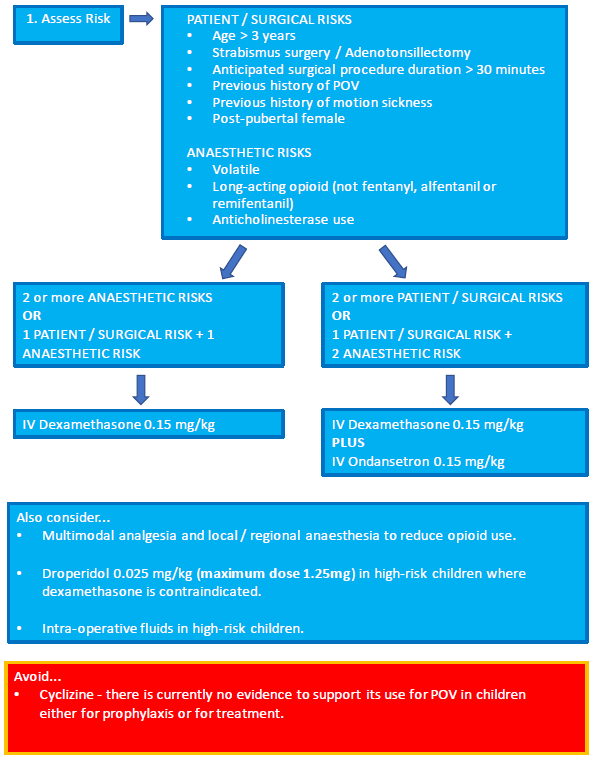
- IV dexamethasone 0.15mg/kg by slow injection
- IV droperidol 0.025mg/kg (maximum dose 1.25mg)
Drug should be diluted and given by slow IV injection if the child is awake
Dexamethasone - Effective anti-emetic in children on its own and in combination with 5HT3 antagonists.
- Multiple small studies have investigated the effect of the dose for PONV - higher doses were associated with no further reduction in PONV and had a higher rate of side effects
- IV dexamethasone may cause perineal warmth and should be injected slowly in the conscious child
- Dexamethasone should not be used in patients at risk of tumour lysis syndrome
|
Droperidol - Used as an antipsychotic and anti-emetic drug for several decades
- Has sedative effects, prolongs the QT interval and can cause extra-pyramidal symptoms
- Effective anti-emetic and relieves nausea singly and in combination. It can be used both as prophylaxis and as rescue therapy.
- Should be diluted in 0.9% NaCl and given as a slow IV bolus
- The use of droperidol is generally confined to rescue therapy or as a second line agent, rather than prophylaxis because of the concerns around sedation and extra-pyramidal side effects
- Contraindicated in patients with known long QT syndrome.
|
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland