 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland
• These should be changed ever 24 hours, at the same time as the PCA syringe.
• Disconnect the PCA syringe giving set fromn the patient’s Venflon.
• Attach the PCA syringe to the new PCA extension set at the anti-reflux valve (Red Valve End).
• Insert the syringe back into the pump and prime the line again, using the priming button on the pump. This ensures that the syringe driver housing is in contact with the syringe barrel.
• Attach the PCA extension set to the patient’s venflon and ensure the blue clamp in unclamped.
• Document in the comments section of the PCA chart the amount (in mls) wasted whilst purging the line.
Patient Controlled Analgesia (PCA) and continuous intravenous morphine infusions (Paediatric Guidelines)

Warning
Morphine Intravenous Infusions/PCA for children may be used on
- Children’s Ward
- Recovery Unit, Theatres
- ITU
- Surgical High Dependency Unit
All PCA infusion/continuous opioid intravenous infusions must be delivered via the Agilia PCA pump
The surgical team should be called in the first instance for all routine surgical problems including: -
- Hypotension
- Nausea and vomiting
- Inadequate analgesia
- Sedation and Respiratory problems
- Urine retention
- Itching
For sedation and respiratory problems the On Call/Duty anaesthetist must also be contacted.
The child should be nursed in the High Dependency Area with continuous pulse oximetry.
The syringe must be connected to the cannula using a PCA administration set which contains an anti-syphon valve to prevent free flow and anti-reflux valve if other fluids are connected to the same venflon.
No other opioids to be administered to the patient whilst, morphine infusion is in use, unless directed by an Anaesthetist or Acute pain nurse.
Ensure Naloxone 400 microgram ampoules are available on the ward.
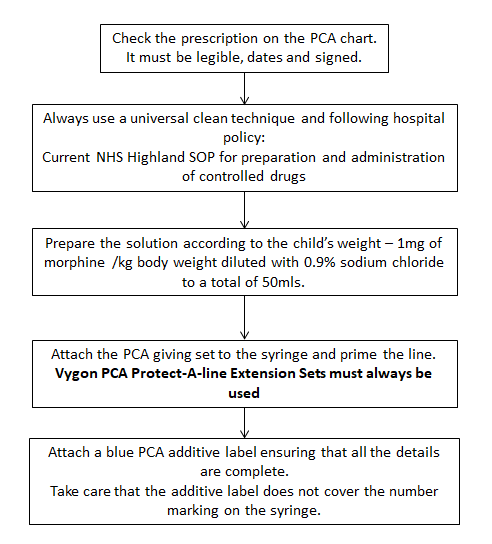
Preparation of Syringe
Preparation of each syringe must be witnessed by a trained nurse or doctor, in accordance with Hospital Policy Preparation and Administration of controlled drugs.
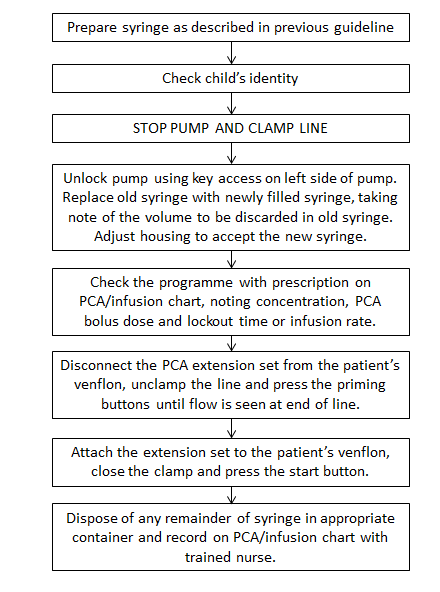
Change of Syringe
Each change of syringe must be witnessed by a trained nurse or doctor who has received PCA training.
Follow the NHS Highland SOP for controlled drug administration.
• Peripheral cannula will be used most commonly but PCA can also be adminstered via central line.
• PCA can be administered on its own but is preferably administered with maintenance fluids to maintain line patency.
• Vygon Protect-A-Line extension set must be used without maintenance fluids and Vygon Protect-A-Line extension set must be used with maintenance fluids.
If the child's pain score > 4 follow below.

Patient Controlled Analgesia should be discontinued when the child no longer requires it, for example.
• An oral route has been established and the patient is able to take oral analgesia.
• The child has required minimal morphine over past 6 hours and has pain score is less than 4 with child able to deep breathe, cough and mobilise.
Note: Changing from PCA to subcutaneous injections is not acceptable when an oral route has been establised. This may only be acceptable when intravenous access is difficult.
• Ensure oral analgesia is prescribed (seek advice from Oral Analgesia chapter before discontinuing PCA/Infusion.
• If child is using large doses of PCA or is poorly controlled on a maximum infusion, please contact Acute Pain Nurse for advice on step-down analgesia.
• Routine pain scoring should continue and be carried out at the same time as the vital observations.
• Switch off pump and clean it as per hospital cleaning policy.
• Ensure handset is cleaned and wrapped around pump.
• Lock pump cover to prevent damage of the cover in transport.
• Place the pump in a clear plastic bag to identify that it has been cleaned.
• Finally, leave it ready for collection or out of hours return the pump promptly to the Equipment Library, Main Theatres.
If a pump is broken or damaged in any way, please send to Medical Physics with a description of the fault. Leave a message on the answer phone at extension 4276.