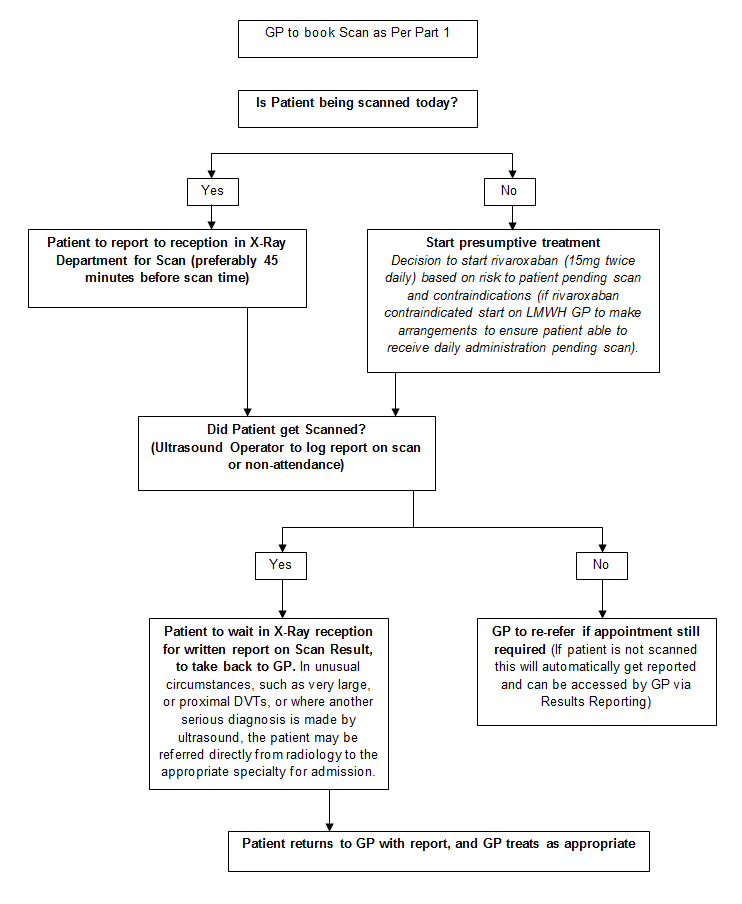
Patients who are considered on clinical grounds as being at moderate or high risk of DVT (Wells’ score -2) and who are not getting ultrasound and follow up the same day should be treated with rivaroxaban pending confirmation of diagnosis.
Initial therapeutic dose (oral): rivaroxaban 15mg twice daily for 21 days then maintentance dose: 20mg once daily thereafter.
Adjustment for renal function (see SPC):
Rivaroxaban is contraindicated if creatinine clearance is less than 15ml/min. Prescribe alternative therapy.
Moderate (CrCl 30 to 49mL/min) or severe (CrCl 15 to 29mL/min) renal impairment: consider reducing maintenance dose from 20 mg once daily to 15 mg once daily if the patient's assessed risk for bleeding outweighs the risk for recurrent DVT and PE. Consider discussing with Haematology.
Mild (CrCl 50 to 80mL/min) renal impairment: no dosage adjustment necessary.
If active malignancy treat with low molecular weight heparin.
Duration of treatment
All patients should be individually assessed for risk: benefit, but the following should be considered:
First DVT confined to below knee clot (or superficial femoral): 6 weeks to 3 months
First DVT, affecting ileo-femoral veins (except superficial femoral): 3 to 6 months. (3 months usually appropriate for temporary risk factors and low risk of recurrence, 6 months for idiopathic DVT or permanent risk factors)
Recurrent DVT (or previous PE): 6 months and consider life-long anticoagulation (usually by switching from Rivaroxaban to Warfarin after 3 months. Discuss with haematology)
Rivaroxaban contraindicated: start enoxaparin subcutaneous injections
Enoxaparin 1.5 mg/kg once daily (rounded to the nearest 10mg) for uncomplicated patients with low risk of venous thromboembolism (VTE) recurrence.
Enoxaparin 1 mg/kg twice daily should be used in all other patients such as those with obesity, symptomatic PE, cancer, recurrent venous thromboembolism (VTE) or proximal thrombosis.
Adjust dose in renal impairment (eGFR less than 30ml/min/1.73m2), see SPCfor details.
If Warfarin therapy to follow LMWH please could the GP complete theWarfarin Referral Form (requires internet access and access to NHS Highland Intranet) and send it to the Anticoagulant Clinic.
If both contraindicated please contact Haematology via Raigmore switchboard (01463 704000).
Graduated compression stockings should be sized and prescribed for all confirmed DVTs, to be worn for 6 months post-diagnosis to reduce the risk of post-phlebetic leg syndrome.
General note: Consider need for investigation of cause of DVT (occult malignancy should be considered, but if there are no warning symptoms, and physical examination (including PR) is normal, further investigation is not usually appropriate. Thrombophilia screening in unexplained events in younger people should be discussed with haematology, and is usually done after anticoagulation warfarin is discontinued).
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland