 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland

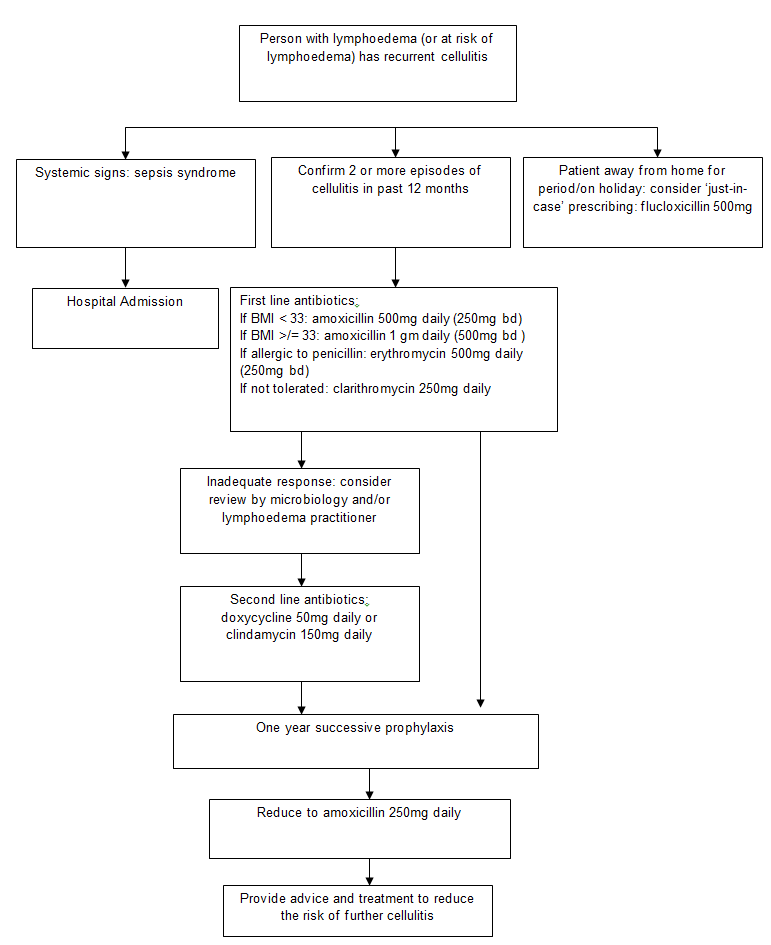
Refer to cellulitis pathway for signs and symptoms, possible investigations and differential diagnosis of cellulitis.
Patient with recurrent cellulitis may be:
- Already diagnosed as having lymphoedema
- At risk of lymphoedema with evidence of possible lymphatic compromise:
- Lymph node removal and/or irradiation
- Obstructive/advanced malignant disease
- Chronic venous disease
- Family history of lymphoedema
- Chronic ulceration, wound infection or inflammatory skin condition damaging local lymphatics.
Additional information:
- Cellulitis is both a symptom and cause of lymphoedema
- Medications such as corticosteroids or cancer treatment, may alter the presentation of cellulitis
- Effective use of decongestive and compression therapy is essential in managing oedema, ulceration and skin problems that may lead to recurrent cellulitis: consider referral to lymphoedema practitioner.