TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland

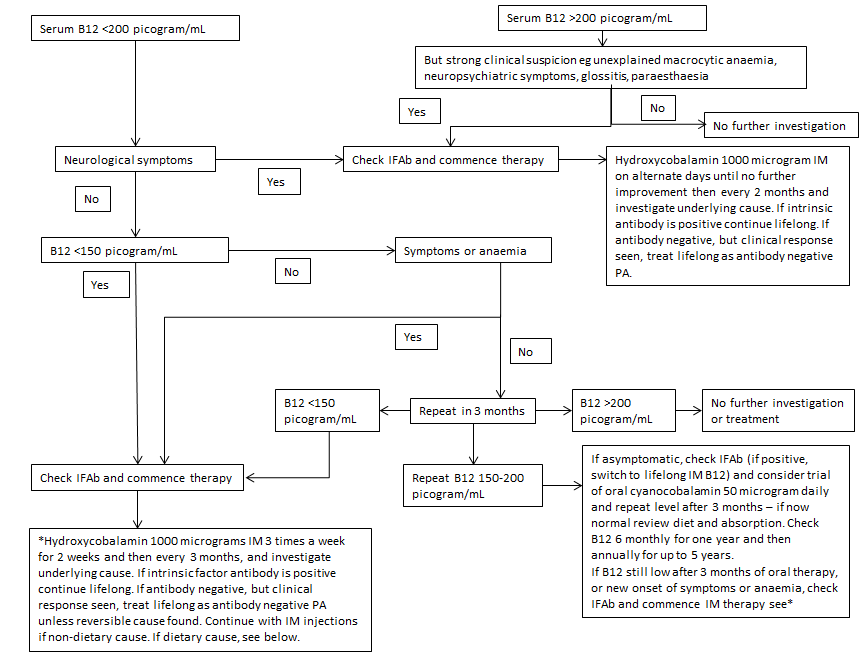
These guidelines are being issued to provide nationally agreed advice for Scotland on appropriate requesting, of B12 testing. B12 testing is often performed indiscriminately as part of routine screening and can lead to unnecessary diagnostic and management quandaries.
Cause of Low B12 levels
- Pernicious anaemia
- vegan diet
- malabsorption syndromes
- coeliac
- sprue
- Crohn's
- ulcerative colitis (UC)
- "food-bound cobalamin malabsorption syndrome" predisposing factors include atrophic gastritis, long term proton pump inhibitor or H2 antagnoist use, chronic alcoholism, gastrectomy/gastric bypass surgery, pancreatic exocrine failure, AIDS
- myeloma (paraprotein related assay interference)
- pregnancy
- combined oral contraceptive pill/HRT
- pancreatric insufficiency
- metformin, acute phase situations