TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland

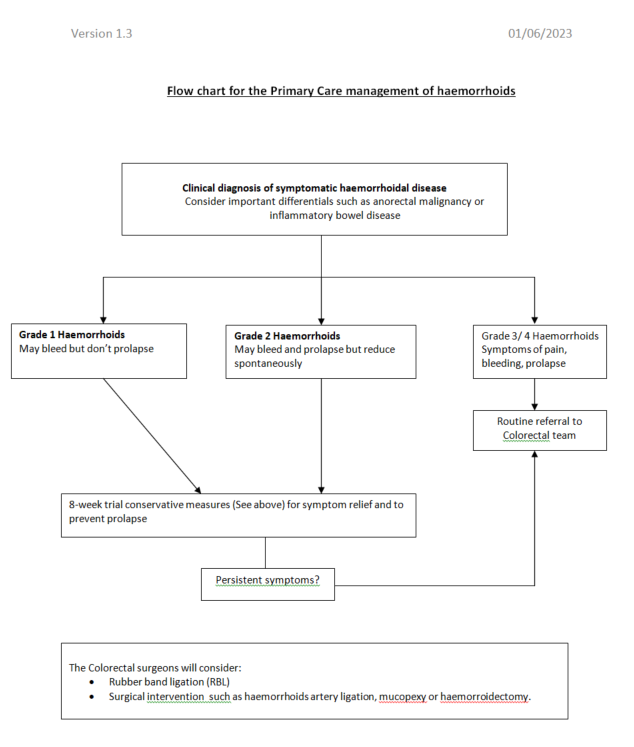
Haemorrhoids are the most common diagnosis of perianal symptoms and a prevalence of up to 44% has been reported in the general population. Within this group, there are many patients with haemorrhoids that are asymptomatic and do not require any of the treatments below.
The majority of haemorrhoids are grade 1 and 2 on the Goligher classification system. According to the European Society of Coloproctologists (ESCP) and the American Society of Colorectal Surgeons (ASCRS) guidelines, conservative measures in primary care are the mainstay of treatment and are aimed at symptom relief and prevention of haemorrhoidal prolapse.