Capacity
In Scotland, parents cannot give consent at all for young people over the age of 16. If they lack capacity, they should be treated under the guidance laid out in the Adults with Incapacity (Scotland) Act 20003.
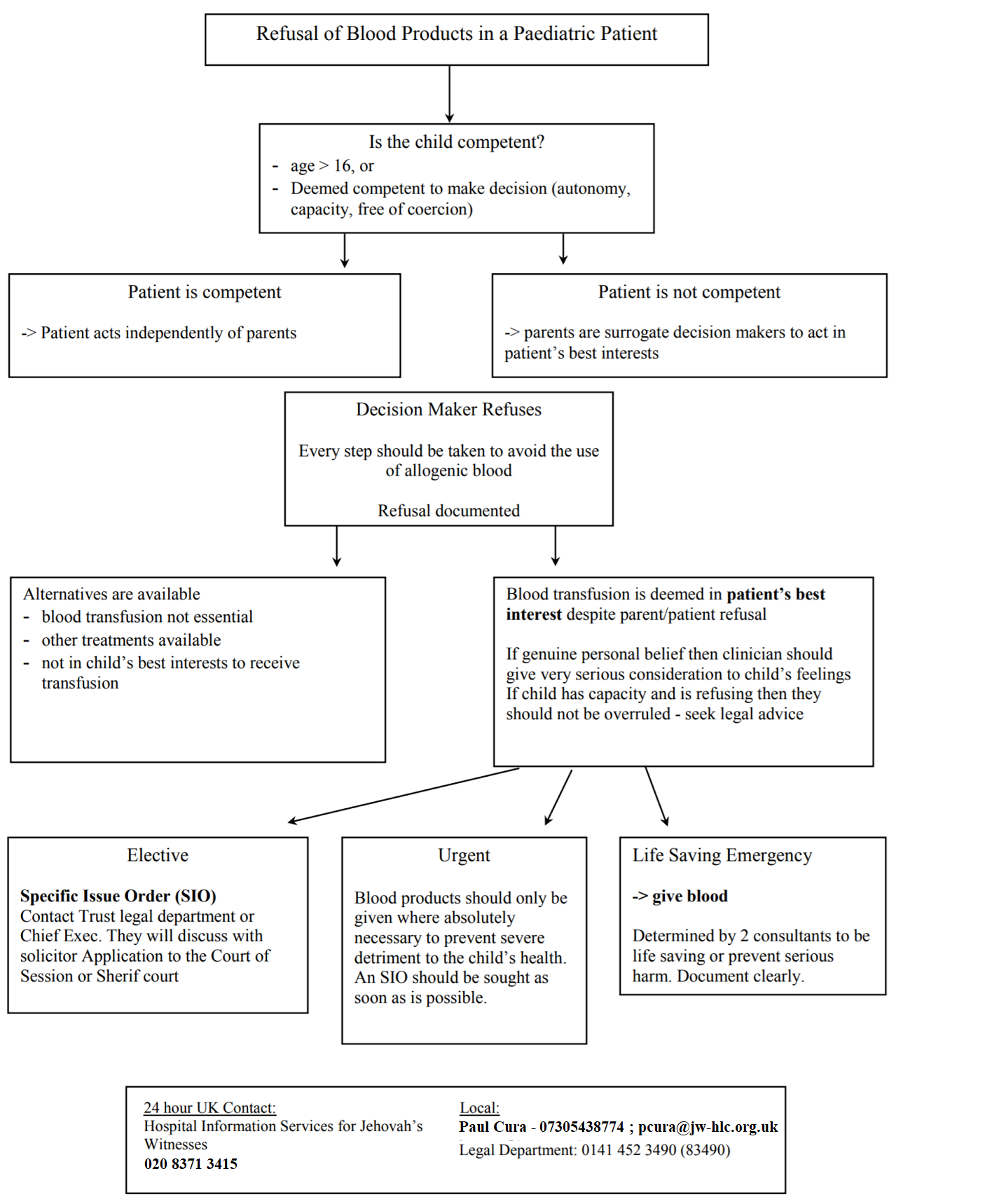
A child under the age of 16 can consent to a procedure if they are deemed by a medical practitioner as capable of understanding the nature and consequences of the procedure [Section 2(4) of the Age of Legal Capacity (Scotland) Act 1991]3. As they are considered to have capacity and be competent then they have the right to refuse treatment and neither the parents nor the court can override it in theory, though this has not be definitively tested in the courts3.
Consent
In addition to capacity, consent requires the decision maker to be fully informed of the risks, benefits and alternatives of the treatment, and for this information to be comprehended. In addition, it is essential that the decision is free from coercion.
Ideally, the discussion regarding administration of blood products should be made remote to theatres with adequate time and privacy. As much as it should be clear that a child with capacity has made the decision of their own reasoning and values, it is similarly important that the medical professional also does not aim to impose undue influence on the decision which is not in keeping with the patient’s own wishes and values.
Emergency
In an emergency blood products can be administered in a life-sustaining situation or to prevent lasting disability without patient or parental consent. Two consultants should agree and document the clinical urgency for blood administration2. Legal permission for treatment in the face of parental refusal should be sought at the earliest available opportunity.
Doctor’s Right to Refuse
Should a medical professional feel they cannot work under the proposed constraints associated with refusal to use blood products, a referral to another appropriately skilled clinical or team should be made and recorded in the notes and an appropriate explanation be given to the family3.