- Bicornuate uterus (heart-shaped womb)
- Unicornuate uterus
- Didelphic (double womb)
- Septate/sub-septate uterus
- Arcuate womb
Women who have had resection of a uterine septum remain at risk of PTB

Please report any inaccuracies or issues with this guideline using our online form
Congenital uterine anomalies (CUA) are malformations of the uterus which occur during development in-utero. These malformations are therefore present from birth and many women have no symptoms-some may experience heavy periods. The implications of CUA, depending on the type and severity, can range from an increased risk of 1st/2nd Trimester miscarriage(s), intra-uterine growth restriction (IUGR), fetal malpresentation, pre-eclampsia and pre-term birth (PTB). There can be an association with anomalies of the genital tract, bladder and kidneys. Consideration should therefore be given to ultrasound imaging of the renal tract if indicated.
To enter a Critical Alert-Woman please search under the ‘Enter new note tab’ (See Picture 1) Complete the boxes (See Picture 2) detailing the details of the alert e.g. Bicornate uterus at EPAS scan.
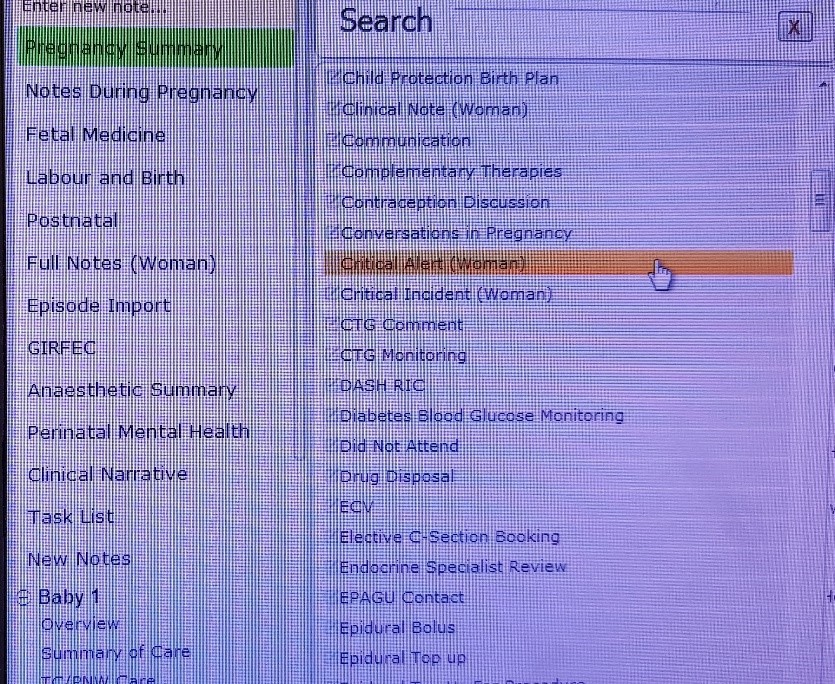
Picture 1
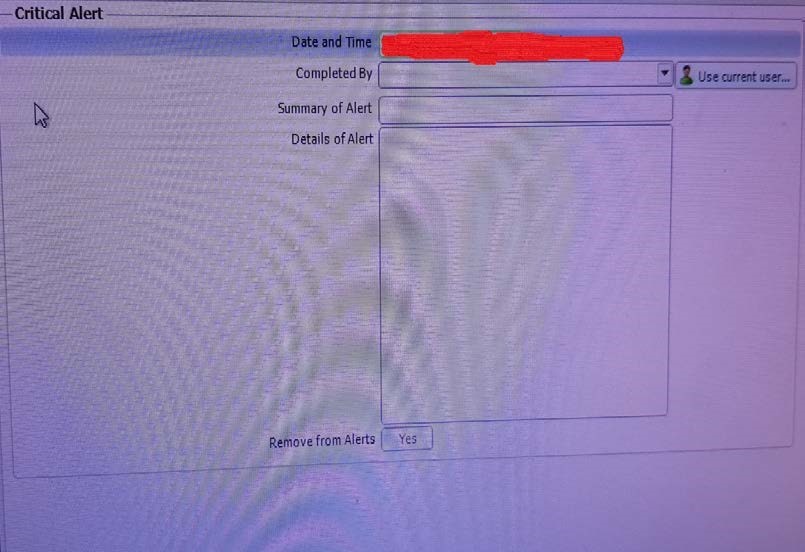
Picture 2
Suggested management includes 3rd trimester growth scans to monitor for IUGR and to confirm fetal presentation by 36 weeks gestation. Women with CUA are advised with signs and symptoms of PTB to contact MAU 24/7 for further assessment. If PTB at <30 weeks gestation is confirmed the Preterm Birth should be followed remembering to include; corticosteroids, Magnesium Sulphate and anti-biotic cover.