A polypharmacy review (following the 7 Steps approach) should ensure optimal management of respiratory conditions, and include addressing aggravating lifestyle factors, consideration of the most appropriate medication at the right dose with regular review.
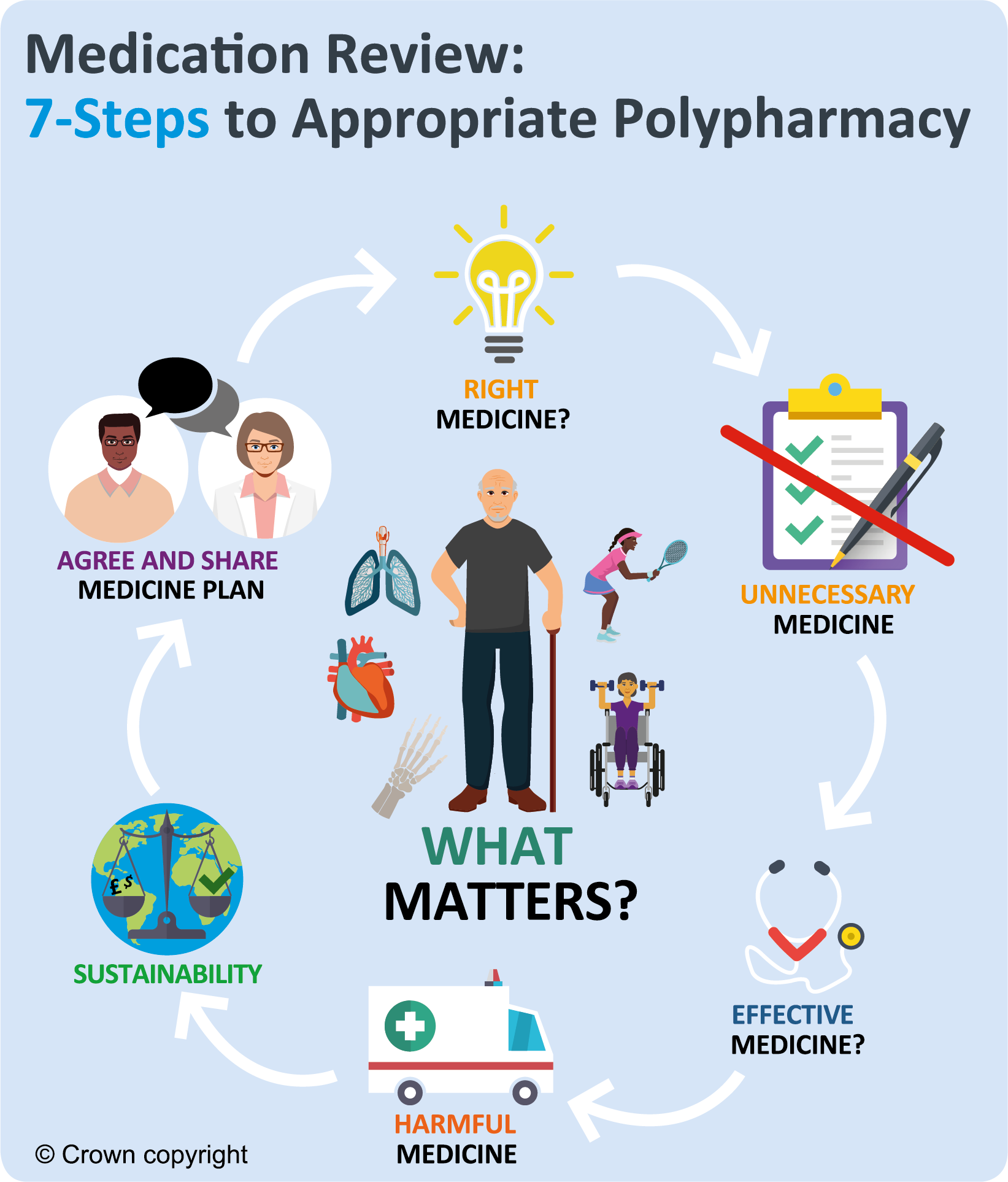
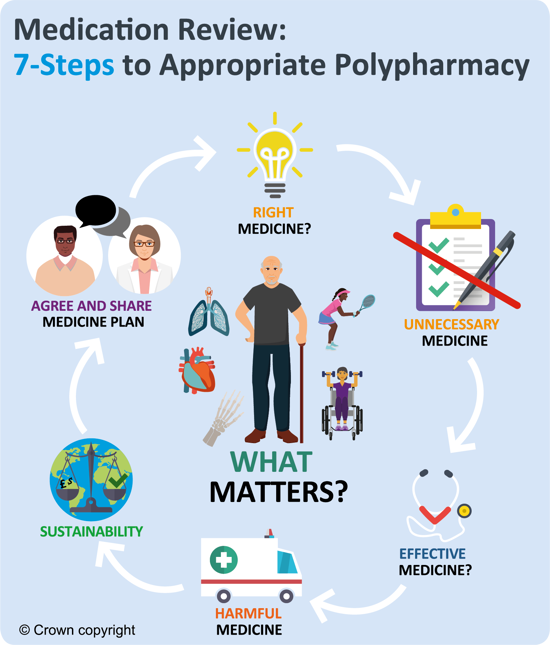
The 7 Steps to appropriate polypharmacy demonstrate that the review process is not a linear single event, but cyclical, requiring regular repeat and review as shown in the image below.
The circle is centred on what matters to the individual, ensuring they are provided with the right information, tools and resources to make informed decisions about their medicines and treatment options.
 Respiratory: Quality prescribing strategy - a guide for improvement
Respiratory: Quality prescribing strategy - a guide for improvement