Management of bleeding with dabigatran
 NHS Borders clinical guidelines
NHS Borders clinical guidelines

Warning
Refer to algorithm
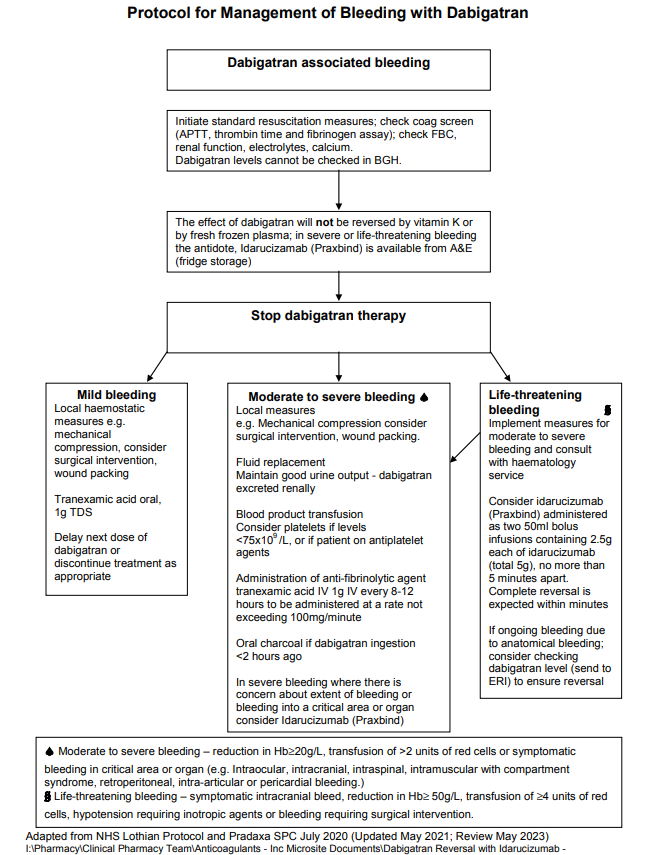
In the event of haemorrhagic complications associated with Dabigatran
- Discontinue dabigatran treatment and investigate the source of bleeding.
- Consideration should also be given to administration of platelet concentrates if
thrombocytopenia is present or long acting antiplatelet drugs have been used. - Initiate appropriate clinical support eg. Surgical or local haemostasis, transfusion of red cells,
volume substitution, inotropic drugs. - When rapid reversal of the anticoagulant effect is required, idarucizumab (Praxbind) is
available in BGH. - Consult haematology if bleeding is moderate to severe or life-threatening.
Consider
- Dabigatran is primarily eliminated in the urine – maintain adequate diuresis.
- The APTT can be used as a qualitative marker of dabigatran activity – if the APTT is normal
dabigatran is unlikely to be present. - Dabigatran has low protein binding and can be dialysed; it may take 6-8 hours to clear
dabigatran this way and limited data supports this approach. The best guide for duration of
dialysis is normalisation of the APTT and/or shortening of the thrombin clotting time to 60
seconds or less. - Absorption of dabigatran can be prevented by the administration of activated charcoal, which
adsorbs toxic substances and reduces or prevents systematic absorption, within 2 hours of
ingestion of dabigatran.