Food bolus obstruction
 NHS Borders clinical guidelines
NHS Borders clinical guidelines

Management of patients
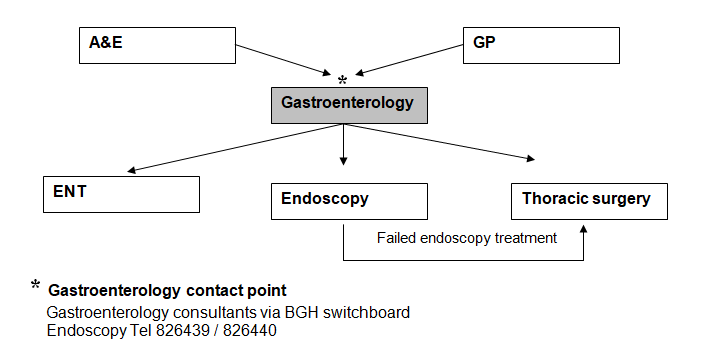
Contact point (in working hours)
The gastroenterology department is best suited to decide on management and should be the contacted first by ED or primary care.
Contact point (out of hours)
If the patient can tolerate the situation overnight then leave nil by mouth on IV fluids and refer to BGH Gastro next morning. If patient distressed or faced with long wait over a weekend ask Gastroenterology registrar at RIE for advice. They may take patient on compassionate grounds for out of hours endoscopy but we do not have a service level agreement in place for such patients.
For foreign body ingestion out of hours contact RIE ENT surgery for foreign body above the sternal notch and Thoracic surgery specialist trainee on call for foreign body below the sternal notch.
Some key facts relating to food bolus obstruction
- The majority of patients will have a structural abnormality and therefore need an urgent endoscopic examination of their oesophagus and stomach even if the food bolus passes spontaneously.
- The patient’s symptoms are an unreliable indicator of site of obstruction.
- Fizzy drinks with or without Buscopan 40mg IV bolus can assist clearing bolus.
- Food bolus obstruction can almost always be treated endoscopically using conscious sedation rather than general anaesthetic.
- Foreign body ingestion is rarer than food bolus and usually requires GA to allow removal. Endoscopy, ENT or thoracic surgery may be involved.
- Sharp edged foreign body needs urgent endoscopic removal before it passes through the pylorus.
Referral route for food bolus obstruction / ingested foreign body