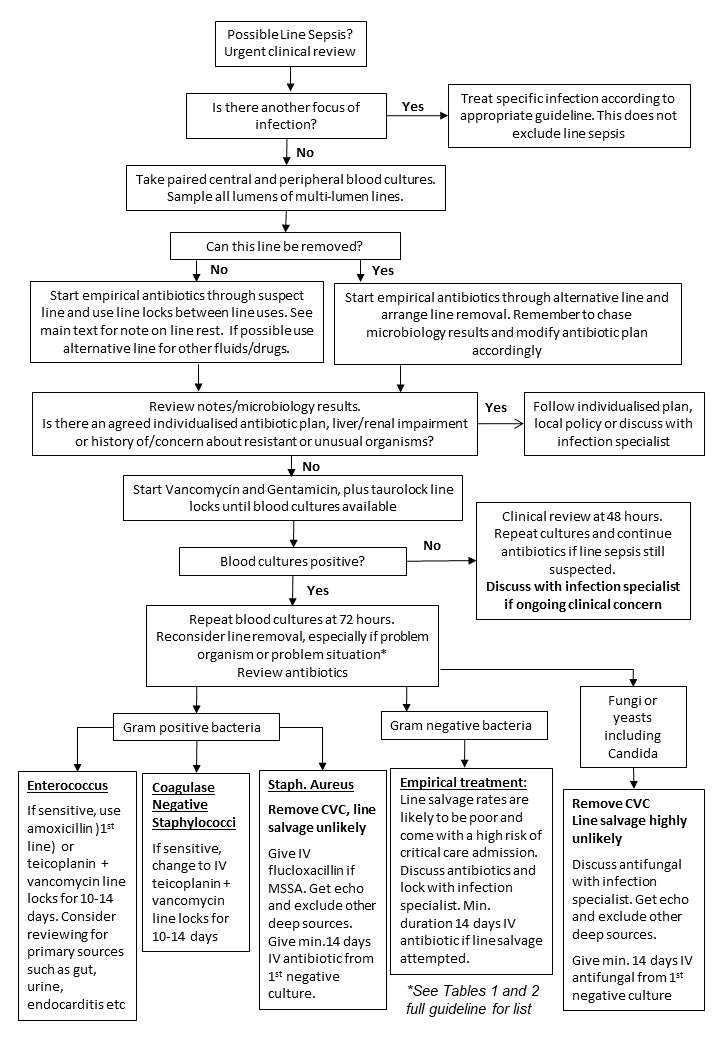
It is recognised that each patient and situation is unique. The following initial actions are recommended in patients with possible or probable line related sepsis:
- Urgent senior clinical review
- Blood cultures (preferably pre-antibiotic)
- Paired line and peripheral blood cultures taken with clear labelling of the request forms
- All lumens of multilumen lines should be sampled separately
- If peripheral cultures are not obtainable, consideration should be given to arterial cultures
- Review for other sources of infection – may require further investigations/imaging etc. Even with an underlying primary source of infection, the line may be secondarily infected.
- Consultation of previous microbiology results – previous resistant or unusual infections may mean that empirical antimicrobials recommended in this guideline or in the therapeutics formulary are inappropriate and alternative regimes may be required. For haemato-oncology and other patients at high-risk of recurrent line infections there may be a condition specific guideline or an existing individualised line infection antibiotic plan which should be followed.
- If in any doubt, early senior clinical review and discussion with an infection specialist should occur
- It is generally against best infection specialist advice to salvage an infected line. However, an early decision regarding salvage, along with institution of lock and systemic antibiotic therapy (through the line to be salvaged) should be made. Where a lock cannot be used, systemic antibiotics should be administered through the line.
- In a patient in whom line sepsis is suspected, and in whom there is a strong reason why line salvage is being considered, line locks and systemic antibiotics down the line should be used. In addition, due to the risk of metastatic septic complications and physiological instability, an early discussion with critical care services is warranted based on level of concern and the species of pathogen isolated. If continued use of the line results in ongoing signs of sepsis then the line should be removed.
- In well patients, single positive cultures with Coagulase Negative Staphylococci might not be significant and these should be repeated prior to initiation of specific therapy.
- Repeat line and peripheral cultures with tailoring of treatment (lock and systemic) to microbiology results are essential if line salvage is attempted. Discuss any antibiotic resistant organisms with an infection specialist. The line should ideally be removed if blood cultures remain positive at 72 hours post initiation of salvage therapy.
- Line removal forms the mainstay of optimal management of these infections. When line sepsis is likely, line tips should be sent for culture and the results chased. If lines are removed but line sepsis is not likely, there is no clinical need to send line tips for culture. In problem situations or when problem organisms are cultured, renewed efforts should be made to remove the line. Certain situations may also prompt a search for other deep sources or metastatic complications (see tables 1 & 2, page 12).
- When line retention and salvage has been attempted using systemic and lock therapy for the recommended durations, line and peripheral cultures should be obtained 48 hours after stopping all antimicrobial therapy