

Juvenile idiopathic arthritis (JIA), management in children (536)

Warning
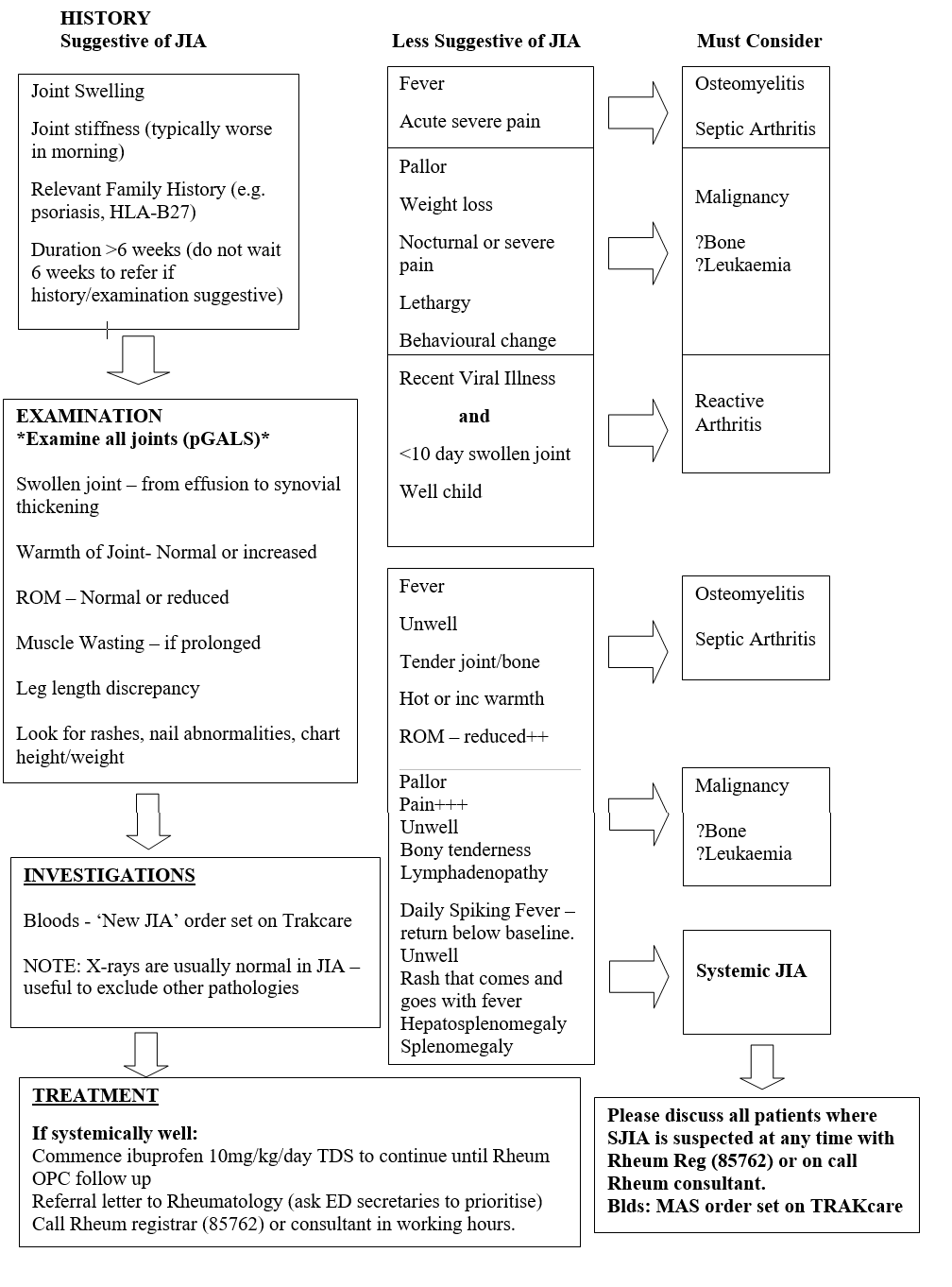
Juvenile Idiopathic Arthritis (JIA) is essentially a diagnosis of exclusion and therefore a high index of suspicion for other differential diagnoses is necessary. The chief differentials for a swollen joint will be infection (septic arthritis or osteomyelitis), malignancy (particularly leukaemia or bone tumours) and trauma.
Note:
- More than one swollen joint will always require rheumatology referral
- In an otherwise well chid with swollen joint(s) the most likely diagnosis is JIA
- Outcome of JIA is better if treated early ∴ have low threshold for referral to Rheumatology
- Beware of labelling all ‘limping’ or non-weight bearing as injury related - some falls are ‘red herrings’. Minor falls are common in children and may be co-incidental.