

- Transplantation undertaken for failed surgical palliation of structural heart disease, cardiomyopathy and occasionally unrepaired congenital lesions
- Delivered at Freeman Hospital ( Newcastle) and Great Ormond Street Hospital (London)
- 20-30 transplants undertaken annually in the United Kingdom, two to three in Scottish recipients
- Rarely more than 10 transplanted children living in Scotland
- Shared care arrangement between Glasgow/Edinburgh and London/ Newcastle
- Follow-up progressively relaxed to six monthly visits in both centres; net three monthly reviews
- Ongoing visits to a distant centre, school and work absence, strict medication regimens, frequent venepuncture, adverse drug reactions, unplanned admissions and a sense of the transplant being life-controlling place heavy burden on patients and families
- Most practitioners are unfamiliar with subtle but sinister clinical signs and in managing acute, unplanned presentations to ED. Parents know this and may be strongly directive during acute presentations
Cardiac transplant patient - paediatric acute care management pathway (1080)

Warning
What's new / Latest updates
06/03/2023 Pathway reviewed with no changes required.
Objectives
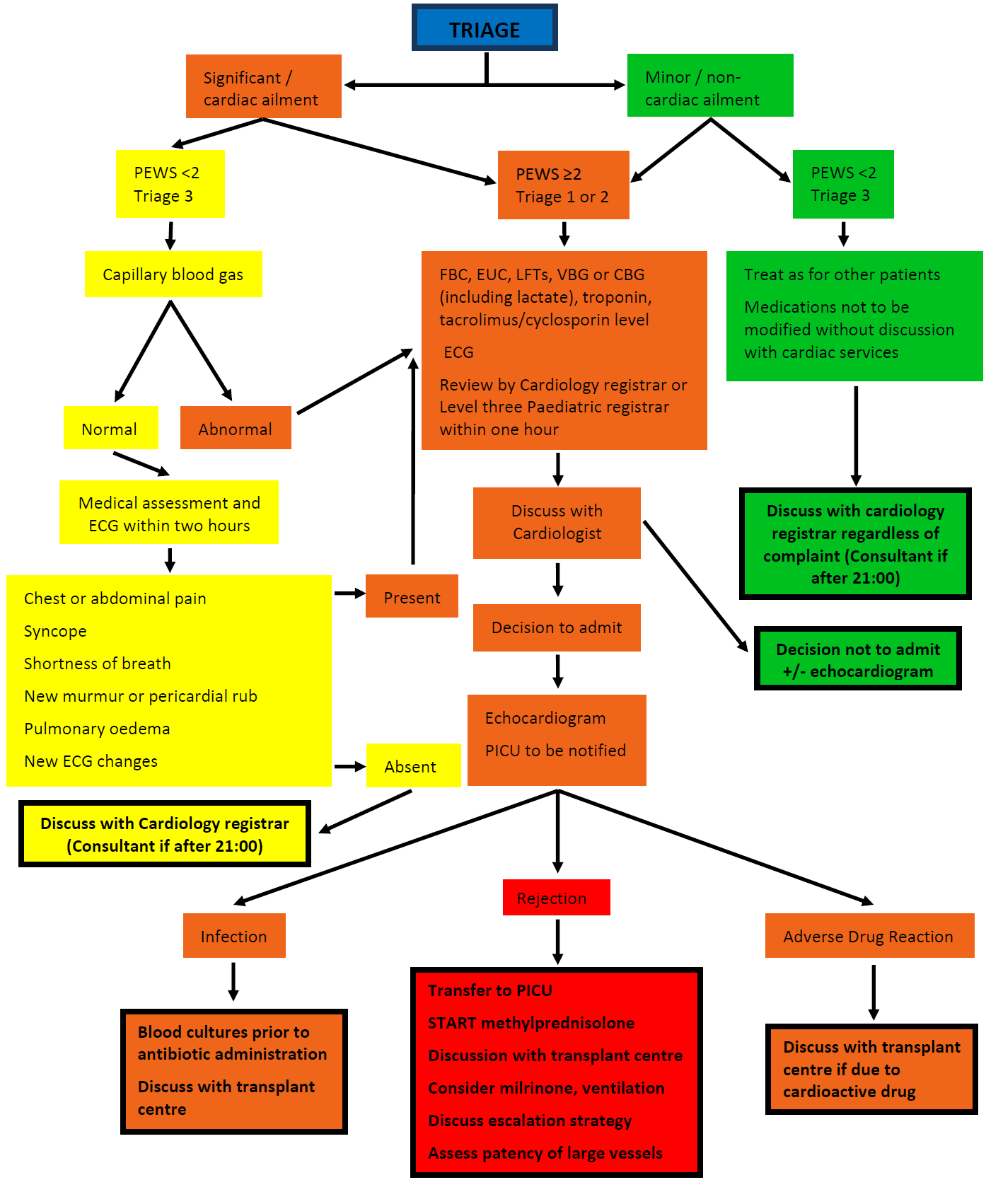
Management of acute presentations of paediatric cardiac transplant patients to the Emergency Department
|
|
Graft rejection
- 20% of patients are treated for rejection in first year after transplant. Risk does not decrease over time
- Asymptomatic, low grade rejection may be detected on routine surveillance biopsy
- Symptoms consistent with reduced cardiac output may be diffuse such as lethargy, fatigue, vomiting and abdominal pain. Chest pain and breathlessness occur later and are very concerning
- May be tachycardia, tachypnoea, gallop rhythm, new murmur, hepatomegaly, chest crackles
- Requires urgent methylprednisolone and potentially antithymocyte globulin, immunoglobulin and plasmapheresis and transfer to transplant centre
Infection
- Immunosuppressed children may show little evidence for infection due to inability to mount immune response; ongoing fever in the absence of signs must be carefully investigated
- Denervated heart does not show a normal chronotropic response to stress and recently transplanted heart may show a high resting rate, slow increase in response to stress and reduced peak rate
- Most infections are bacterial, followed by viral; risk is highest in the first year following transplant
- Fever may also indicate graft rejection or malignancy
Adverse drug reactions
- Calcineurin inhibitor such as cyclosporine or tacrolimus prescribed as primary immunosuppression. Dosing based on trough serum levels; narrow therapeutic window. May cause hypertension, IDDM, renal dysfunction, dyslipidaemia , hypomagnesaemia and hyperkalaemia
- Mycophenylate mofetil (MMF) as a secondary agent. Causes gastrointestinal upset
- Variable dose of prednisolone is usual; standard steroid adverse effects
- Frequently an antihypertensive, iron and vitamin supplements, a statin and prophylactic azithromycin
- Aggressive immunosuppression causes recurrent infections and malignancies, in particular post-transplant lymphoproliferative disease (PTLD)
- Lighter immunosuppression associated with graft rejection and accelerated coronary vascular disease
- Accelerated coronary artery disease; diffuse stenoses secondary to chronic immune rejection and effects of diabetes (drug-induced), hypertension and dyslipidaemia. Leading cause of graft loss; only definitive treatment is re-transplantation
- PTLD seen in immunosuppressive-induced high EBV viral titres. Presentation highly variable; lymphadenopathy or adenotonsillar hypertrophy in the setting of recurrent fever, weight loss, fatigue or other unexplained symptoms is concerning