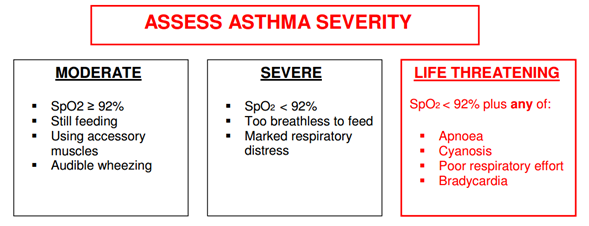
- If a patient has symptoms and signs across categories, always treat according to their most severe features
- Most infants have recession with audible wheeze but are not distressed
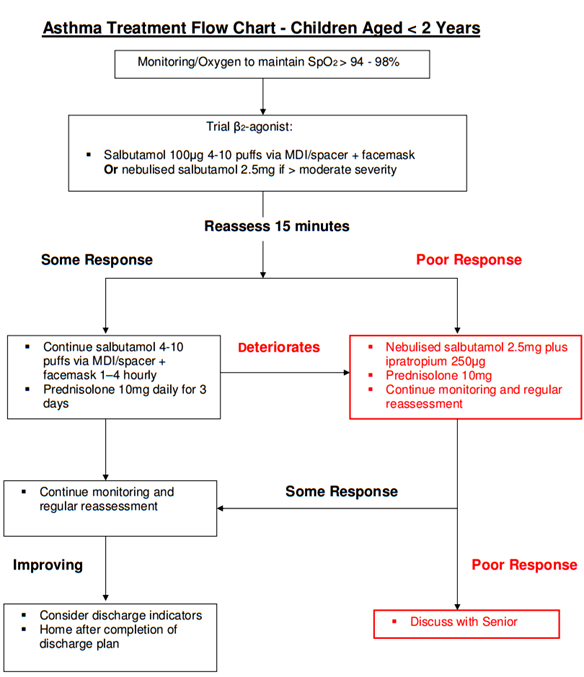
- MDI + facemask/spacer is as effective as, if not better than, nebulisers for treating mild to moderate asthma in children aged < 2 years
- Steroid tablets in conjunction with β2-agonists have been shown to reduce hospital admission rates when used in the ED