1. Emergency treatment Recommendations for life-threatening bleeding in women with ITP
A combination of initial treatments, including IV corticosteroids and, usually, IVIg, should be used in emergency situations in which there is an urgent need to increase the platelet count within 24 hours. Platelet transfusions may be helpful and must not be postponed in cases of life-threatening bleeding, especially haemorrhage. In the case of life-threatening bleeding and the absence of a significant response to IVIg and platelet transfusion in a patient on corticosteroids, the use of a TPO-RA should be considered. Additional options may include vincristine or vinblastine, antifibrinolytics in combination with other initial therapies, and, rarely, emergency splenectomy.
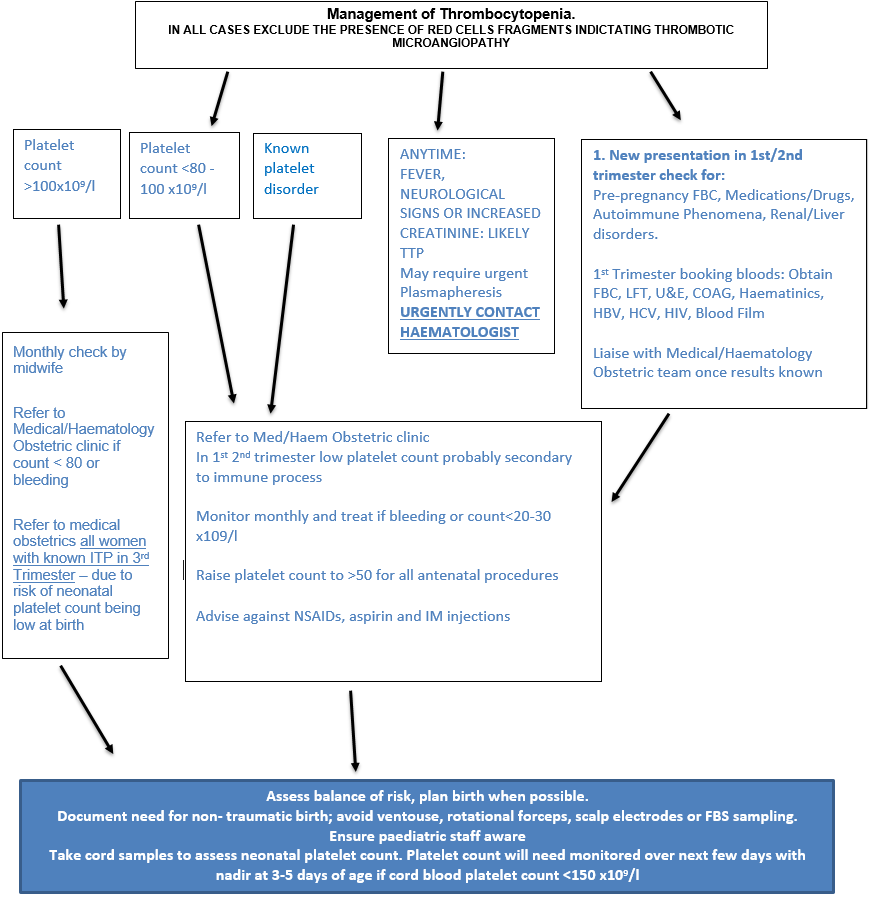
Below are recommendations for the management of ITP during pregnancy, but a haematologist should always be consulted in such cases.
2. Recommendations for the treatment of maternal ITP
1. Counselling for women with ITP wishing to become pregnant is recommended.
2. A platelet count between 20-30 x 109 /L in a non-bleeding patient is safe for most of pregnancy. A platelet count ≥ 50 x109 /L (see separate anaesthesia recommendation above) is required for delivery.
3. Initial treatment is with oral steroids or IVIg.
4. IVIg can provide a rapid, but often very transient, increase in platelet count and can be used to urgently increase platelet counts during bleeding or for delivery.
5. Combining therapies may elicit a response in patient’s refractory to single agents alone. High-dose methylprednisolone, in combination with IVIg and/or azathioprine, is suggested for ITP refractory to oral corticosteroids or IVIg alone.
6. Rituximab can be considered in pregnancy for very severe cases, but perinatal and neonatal immunosuppression and subsequent infection are potential complications and require monitoring.
7. TPO-RAs may be considered in late pregnancy when other treatments have failed, but published information is limited.
8. In the rare instances when splenectomy is required, it should be performed in the second trimester.
9. Vinca alkaloids, danazol, and immunosuppressive drugs not listed in these recommendations should be avoided in pregnancy.
3. Recommendations for management of birth of newborn infants to mothers with ITP
1. Neonatal alloimmune thrombocytopenia should be excluded by parental testing if the neonate presents with severe thrombocytopenia.
2. The mode of birth should be determined by obstetric indications, not by anticipation of the neonatal platelet count.
3. Procedures during labour that may be associated with increased hemorrhagic risk to the fetus should be avoided, specifically the use of fetal scalp electrodes, fetal blood sampling, assisted vaginal birth with ventouse, and assisted vaginal birth with rotational forceps.
4. Previous maternal splenectomy can be associated with a higher risk for neonatal thrombocytopenia even if the mother now has a normal platelet count.
5. A mother with a previous newborn, thrombocytopenic or not, is likely to have a second baby with a similar platelet count. Umbilical cord platelet count should be obtained at the time of birth or as soon as possible afterwards
6. Repeat the platelet count as needed depending on platelet levels, trends in the count, and response to treatment (if any). If cord platelet count is ≤ 150 x 109 /L, repeat the platelet count daily until stable. The incidence of pseudothrombocytopenia is high in neonates because of the difficulties encountered in obtaining unclotted blood with blood draws.
7. If platelet count is ≤ 50 x 109 /L at birth, perform a cranial ultrasound. Magnetic resonance imaging for confirmation or clarification can be performed without anaesthesia using the sleep and swaddle approach 30 to 60 minutes prior.
8. In the case of ICH, give IVIg and limited steroids to maintain platelet count ≥ 100 x 109 /L for 1 week if possible and ≥ 50 x 109 /L for another week. The use of platelet transfusion may increase neonatal risk.
7. If there is symptomatic bleeding or if platelet count is ≤ 30 x 109 /L, with or without platelet transfusion, give IVIg.
8. If severe thrombocytopenia continues for 1 week in a breast-fed infant, consider pausing breastfeeding for a few days to see whether platelet count increases.