 Diabetes & endocrinology
Diabetes & endocrinology
In hospital, the capillary blood glucose (CBG) target is 6-12 mmol/L.
In the community people will have individualised CBG targets.
If CBG is consistently >12 mmol/L, this needs assessed and addressed, and treated urgently if >16.

In hospital, the capillary blood glucose (CBG) target is 6-12 mmol/L.
In the community people will have individualised CBG targets.
If CBG is consistently >12 mmol/L, this needs assessed and addressed, and treated urgently if >16.
Step 1: Look at current diabetes medication
Step 2: Consider addition of oral medication
Step 3: Consider correction dose of short acting insulin (e.g. novorapid)
(INPATIENT ONLY - IN COMMUNITY CONTACT DIABETES TEAM ON CALL AT THIS POINT)
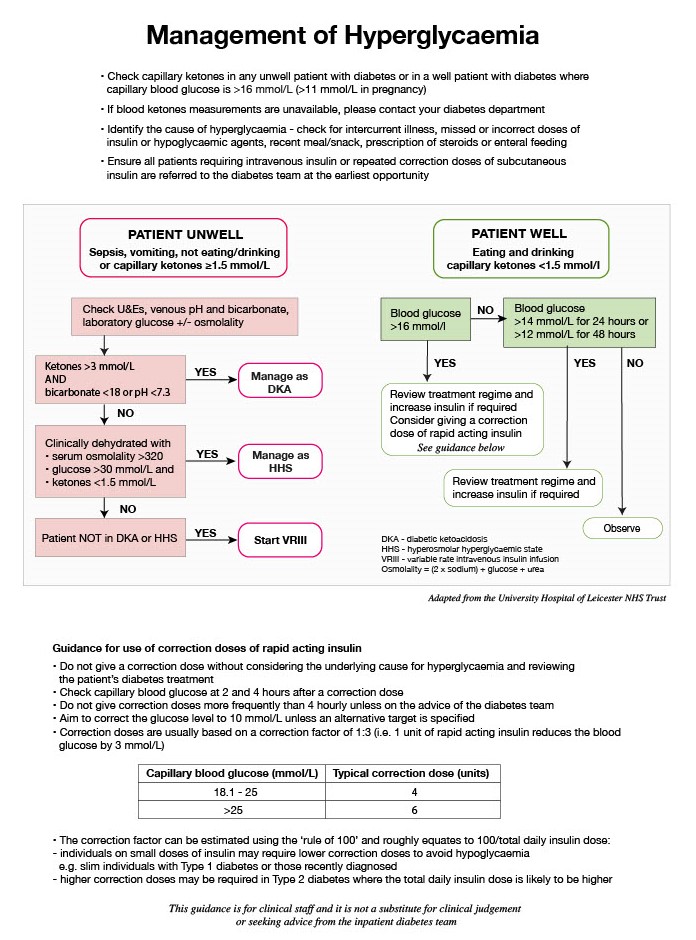
Please use insulin titration advice.
1: please do not give a correction dose more than every 4 hours
2: please contact diabetes team if you are needing to give more than 2 correction doses as regular treatment will need to be reviewed