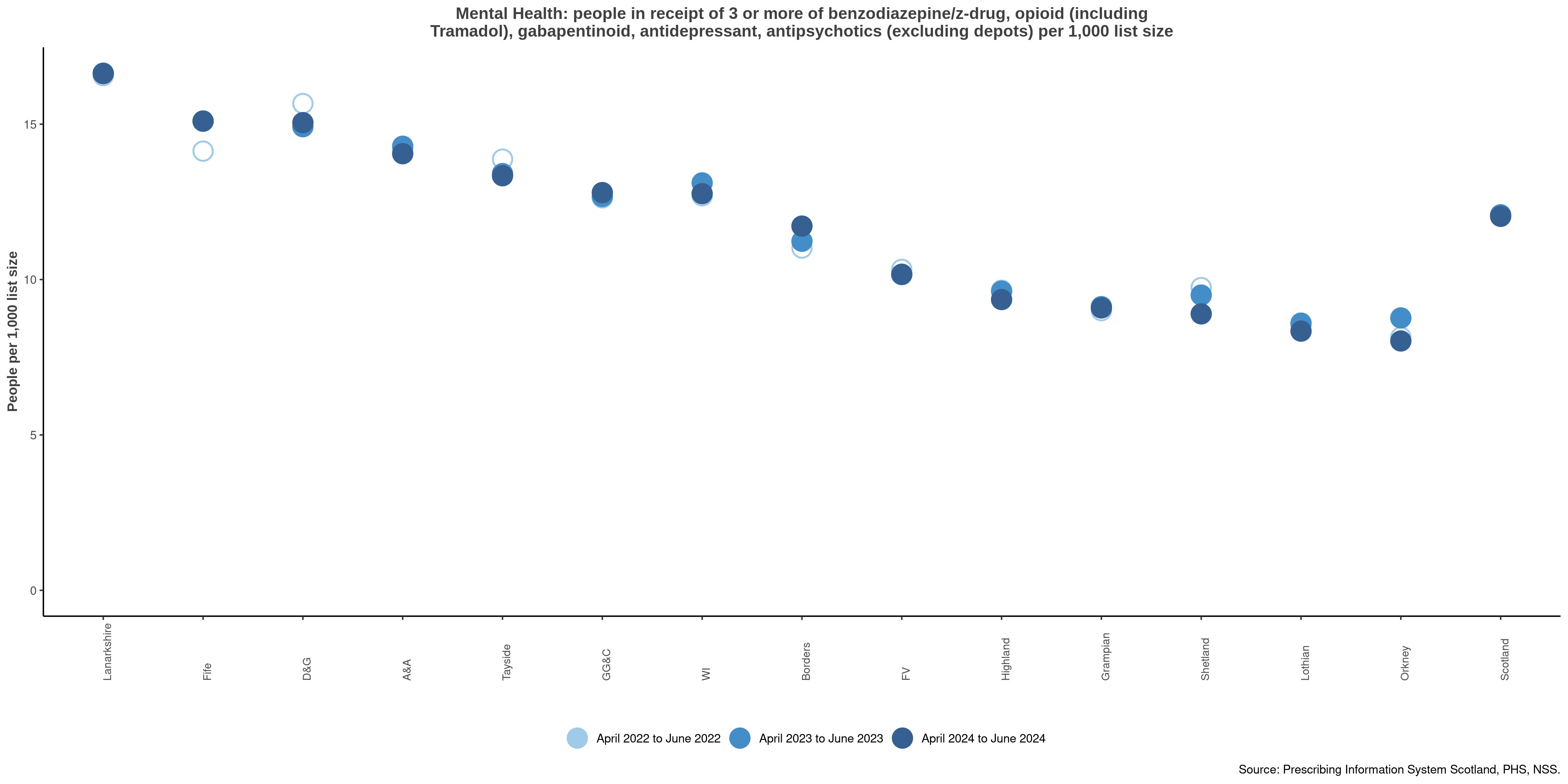
NTI: Mental health triple whammy – All people in receipt of three or more of benzo/ Z-drug, strong opioid (including tramadol), gabapentinoid, antidepressant, antipsychotics (excluding levomepromazine 6mg tabs or injections) per 1,000 list size
Click on the chart to view a larger version.

The combination of three or more of these medications increases the risks of medicine-related harm. Prescribers should consider the ‘benzo-burden’ – the total benzodiazepine-type drug load prescribed per day – as benzodiazepines, z-drugs and gabapentinoids have similar synergistic effects: sedation, respiratory depression, etc. These may interact with an individual’s conditions to cause more adverse effects and avoidable medicine-related harms e.g. increased breathlessness, fatigue, respiratory depression which can be potentially fatal.
- Opioids: the effects of B-Z and the ‘benzo-burden’ can be further be exacerbated by the addition of a range of opioids, and even reduce the protective ceiling effects of buprenorphine. MHRA advice is only prescribe B-Z and opioids together if there is no alternative and closely monitor individuals for signs of respiratory depression.
- B-Z use with antipsychotics is associated with a higher mortality risk for people with schizophrenia.
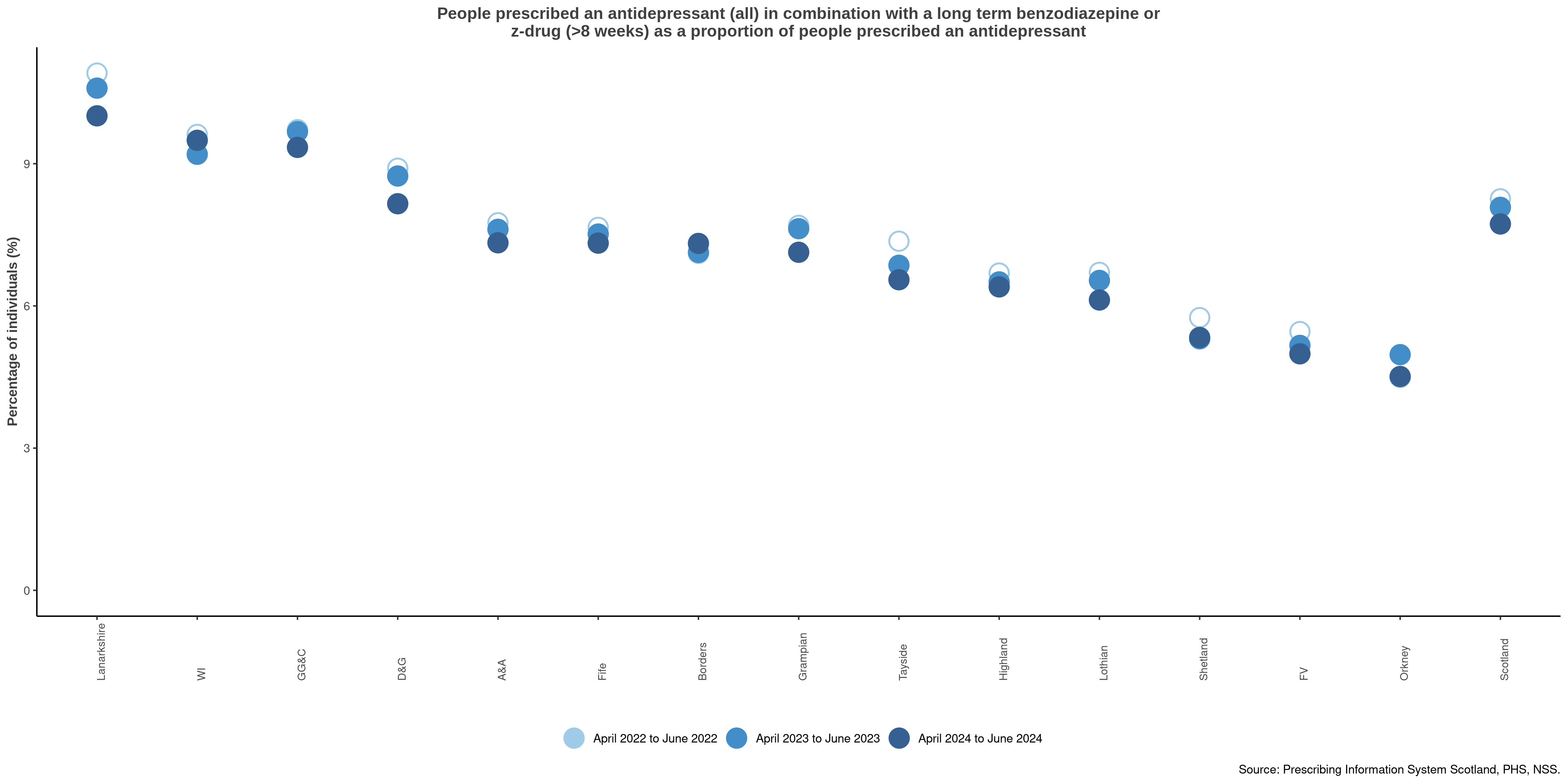
- B-Z use with antidepressants: the use of SSRIs, and particularly high dose SSRIs for the treatment of depression. This may cause more avoidable adverse effects and harms such as anxiety, agitation and insomnia. However, B-Z are also associated with an increased incidence of depressive symptoms, so reviewing and reducing B-Z use may help to optimise care and recovery.
People who report/present with street/non-prescribed B-Z use, often set within the context of polysubstance use, are arguably at greatest risk of combination effects.
This indicator should have a high percentage, indicating alignment with current best practice prescribing guidance.
Actions
- Health boards and prescribers to ensure appropriate use of B-Z in conjunction with other medication; promoting person-centred reviews, and appropriate continuation, reduction and stopping
- The 'What matters to you' approach should assist the individual to achieve goals which have been identified and developed in partnership with clinicians
- The long-term B-Z should be reviewed.
- where appropriate gradually withdraw using an agreed structured and planned reduction schedule
- a small minority of individuals may require longer-term B-Z treatment with regular review to optimise care and minimise street/illicit B-Z use
- Consider pain management and ensure valid indication for analgesia, e.g. neuropathic pain, nociceptive pain. If no ongoing indication for opioid or gabapentinoids, reduce gradually to prevent withdrawal
- Review duration of treatment for depression, and if ongoing need. If none, reduce gradually to prevent discontinuation effects
- Non-pharmacological options, including psychosocial and/or psychological interventions, should be encouraged and pursued where appropriate, e.g. regular physical activity, cognitive behavioural therapy
- Review effectiveness, tolerability and compliance on an ongoing basis
- The 7-Steps review process should be used for all medication reviews
- The Scottish Drug Deaths Taskforce and Public Health Scotland’s: Medication Assisted Treatment (MAT) standards informed response for benzodiazepine harm reduction guidance:
- highlights that everyone has a responsibility to respond to B-Z related harms and to have supportive, collaborative conversations regarding B-Z
- supports a comprehensive, holistic assessment of need to develop a psychological formulation of the presenting issues to inform highly intensive, flexible and individualised care plans
- supports addition of psychological components of care, to support harm reduction and stabilisation
- Individuals can be identified using the Scottish Therapeutics Utility (STU) in GP practices
Notes:
- Levomepromazine not included as generally used in palliative care.
- Opioids include: buprenorphine, fentanyl, morphine, oxycodone (with/without naloxone), pentazocine, tapentadol, hydromorphone, pethidine, methadone, tramadol (with/without paracetamol)
- Benzodiazepines and z-drugs include: Diazepam, Chlordiazepoxide, clonazepam, loprazolam, lorazepam, lormetazepam, oxazepam, nitrazepam, temazepam, alprazolam, clobazam, flurazepam, zolpidem, zopiclone, zaleplon
Formulations excluded: injectables (B-Z and opiate pain medicines), suppositories and enemas (benzodiazepines).
 Benzodiazepines and z-drugs: Quality prescribing - a guide for improvement
Benzodiazepines and z-drugs: Quality prescribing - a guide for improvement