Depression with anxiety
 Benzodiazepines and z-drugs: Quality prescribing - a guide for improvement
Benzodiazepines and z-drugs: Quality prescribing - a guide for improvement
Background (age, sex, occupation, baseline function)
- 49-year-old female
- Works two part-time jobs: school cleaner and dinner lady at different schools
- Lives with adult daughter (currently pregnant) and daughter's partner
- Two adult sons, one local, one lives further away
- Very active helping others
History of presentation/reason for review
- Contacted by the practice for review of her benzodiazepine
Current medical history and relevant co-morbidities
- Mixed depression anxiety – 20 years
- Asthma – 20 years
- Dry eyes – 2 years
Current medication and drug allergies (include OTC preparation and herbal remedies)
- Carbomer eye gel - as required
- Clenil® (beclomethasone) 200 microgram MDI - two puffs twice daily
- Hypromellose eye drops - as required
- Diazepam 5mg tablets - two tablets three times a day
- Paracetamol 500mg tablets - two tablets four times a day if needed
- Salbutamol 100microgram MDI - one to two puffs four times a day if needed
- Temazepam 20mg tablets – one tablet at night
- Venlafaxine 150mg modified-release (MR) capsules – one capsule daily (prescribed for three years)
Lifestyle and current function (including frailty score for >65yrs) alcohol/smoking/diet/physical activity
- Walks between jobs, does not drive
- Smoker - 10 cigarettes per day
- No alcohol
- Number of episodes of deliberate self-harm, last overdose five years ago
“What matters to me” (patient ideas, concerns and expectations of treatment)
- Main focus is being there for and able to help her family
- At review agrees to reduce diazepam but not temazepam
- Managing well with other medicines, reports:
- Asthma well controlled (Has ordered two salbutamol reliever inhalers over last 12 months). Demonstrates good inhaler technique
- Depression and anxiety mood stable, less depression symptoms over the last two to three years. PHQ-9 score 8 (mild depression). Denies thoughts of self-harm or suicide
- Invite individual to complete questions to prepare for the review (PROMs)
Results e.g., biochemistry, other relevant investigations or monitoring
Note: local lab reference ranges may vary
- Weight 52kg, height 1.6m, BMI 20 kg/m2
- BP 134/84 mmHg
- Normal blood results previously, including thyroid function tests
Most recent relevant consultations
- Rarely attends GP. Last consultation 18 months ago for dry eyes
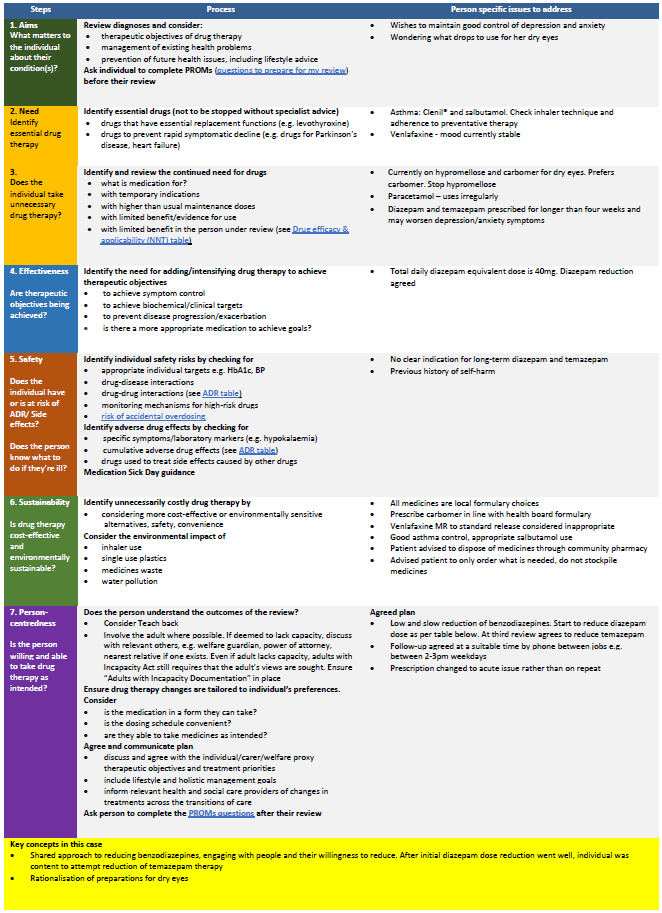
7 Steps: Person specific issues to address for case study
1. Aims: What matters to the individual about their condition(s)?
Review diagnoses and consider:
- Therapeutic objectives of drug therapy
- Management of existing health problems
- Prevention of future health issues, including lifestyle advice
- Ask individual to complete Patient Reported Outcomes Measures (PROMS) before the review
Person specific actions
- Wishes to maintain good control of depression and anxiety
- Wondering what drops to use for her dry eyes
2. Need: Identify essential drug therapy
Identify essential drugs (not to be stopped without specialist advice*)
- Drugs that have essential replacement functions
- Drugs to prevent rapid symptomatic decline
* with advice from healthcare professional with specialist interest
Person specific actions
- Asthma: Clenil® and salbutamol. Check inhaler technique and adherence to preventative therapy
- Venlafaxine - mood currently stable
3. Does the patient take unnecessary drug therapy?
Identify and review the continued need for drugs
- what is medication for?
- with temporary indications
- with higher than usual maintenance doses
- with limited benefit/evidence for use
- with limited benefit in the person under review (see Drug efficacy & applicability (NNT) table)
Person specific actions
- Currently on hypromellose and carbomer for dry eyes. Prefers carbomer. Stop hypromellose
- Paracetamol – uses irregularly
- Diazepam and temazepam prescribed for longer than four weeks and may worsen depression/anxiety symptoms
4. Effectiveness: Are therapeutic objectives being achieved?
Identify the need for adding/intensifying drug therapy to achieve therapeutic objectives
- to achieve symptom control
- to achieve biochemical/clinical targets
- to prevent disease progression/exacerbation
- is there a more appropriate medication to achieve goals?
Person specific actions
- Total daily diazepam equivalent dose is 40mg. Diazepam reduction agreed
5. Safety: Does the individual have or is at risk of ADR/ side effects? Does the patient know what to do if they’re ill?
Identify individual safety risks by checking for
- appropriate individual targets
- drug-disease interactions
- drug-drug interactions (see ADR table)
- monitoring mechanisms for high-risk drugs
- risk of accidental overdosing
Identify adverse drug effects by checking for
- specific symptoms/laboratory markers
- cumulative adverse drug effects (see ADR table)
- drugs used to treat side effects caused by other drugs
Medication Sick Day guidance
Person specific actions
- No clear indication for long-term diazepam and temazepam
- Previous history of self-harm
6. Sustainability: Is drug therapy cost-effective and environmentally sustainable?
Identify unnecessarily costly drug therapy by
- considering more cost-effective alternatives, safety, convenience
Consider the environmental impact of
- Inhaler use
- Single use plastics
- Medicines waste
- Water pollution
Person specific actions
- All medicines are local formulary choices
- Prescribe carbomer in line with health board formulary
- Venlafaxine MR to standard release considered inappropriate
- Good asthma control, appropriate salbutamol use
- Patient advised to dispose of medicines through community pharmacy
- Advised patient to only order what is needed, do not stockpile medicines
7. Patient centeredness: Is the patient willing and able to take drug therapy as intended?
Does the person understand the outcomes of the review?
- Consider teach-back
- Involve the adult where possible. If deemed to lack capacity, discuss with relevant others, e.g. welfare guardian, power of attorney, nearest relative if one exists. Even if adult lacks capacity, adults with Incapacity Act still requires that the adult’s views are sought. Ensure “Adults with Incapacity Documentation” in place
Ensure drug therapy changes are tailored to individual’s preferences. Consider
- is the medication in a form they can take?
- is the dosing schedule convenient?
- what assistance is needed?
- are they able to take medicines as intended?
Agree and communicate plan
- discuss and agree with the individual/carer/welfare proxy therapeutic objectives and treatment priorities
- include lifestyle and holistic management goals
- inform relevant health and social care providers of changes in treatments across the transitions of care
Ask individual to complete post-review PROMS questions after their review
Agreed plan
- Low and slow reduction of benzodiazepines. Start to reduce diazepam dose as per table below. At third review agrees to reduce temazepam
- Follow-up agreed at a suitable time by phone between jobs e.g. between 2-3pm weekdays
- Prescription changed to acute issue rather than on repeat
Key concepts in this case
- Shared approach to reducing benzodiazepines, engaging with people and their willingness to reduce. After initial diazepam dose reduction went well, individual was content to attempt reduction of temazepam therapy
- Rationalisation of preparations for dry eyes
Click on the table image to view a PDF version of the full 7 steps table for depression with anxiety case study.