Antimicrobial prescribing: NHS Lothian
Antimicrobial prescribing: NHS Lothian

Rationale for de-labelling penicillin allergies
- 10% of hospital inpatients have a documented allergy to penicillin.
- 90% of these are not truly penicillin allergic.
- Using non beta-lactam* based antibiotics can be associated with harm including worse outcomes from the infection being managed and additional toxicity from the antibiotics used.
- De-labelling allows you to use penicillin antibiotics for the current infection (and future infections).
- Further information in the format of FAQs is available here.
Safety of de-labelling
- Many patients who report an allergy actually have an intolerance or side effect and can be safely de-labelled without further assessment.
- The penFAST tool has been validated in identifying low risk penicillin allergy patients who are suitable for de-labelling.
- Oral penicillin challenge has been shown to be equally safe and effective as skin testing in low risk patients.
- Delayed reactions post challenge can occur although these are uncommon and generally mild.
Who can assess a penicillin allergy?
- A penicillin allergy history and penFAST score can be undertaken by all clinical staff.
- Direct de-labelling can be undertaken by all prescribers using the guidance below.
- Oral penicillin challenge should only be undertaken by prescribers after consulting with the senior clinician responsible for the patient.
What settings can the de-labelling protocol be used in?
- This protocol can be used in both outpatient and inpatient secondary care settings where resuscitation equipment, and staff trained in its use are available. This includes hospital wards, outpatient departments, critical care and emergency departments.
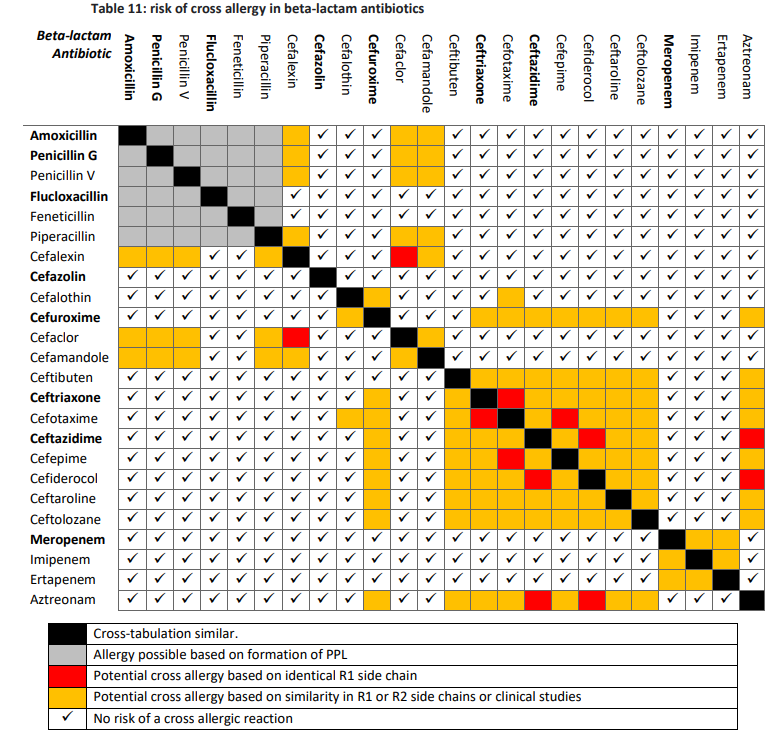
* A summary of which antibiotics are in the beta-lactam group can be found in the "Antimicrobial prescribing for patients with penicillin allergy" section at the bottom of this page