Antidepressants: Quality prescribing - a guide for improvement
Antidepressants: Quality prescribing - a guide for improvement
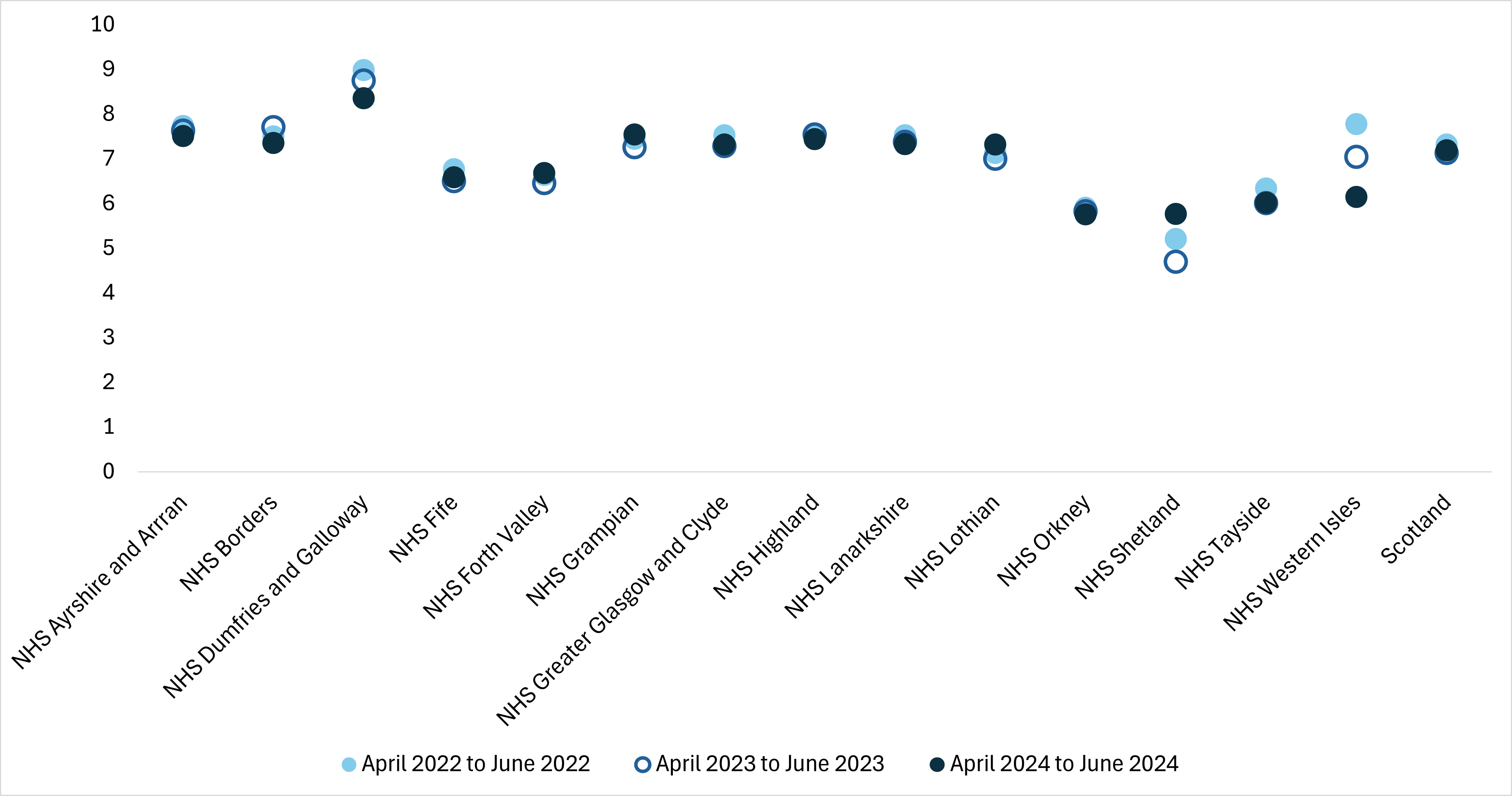
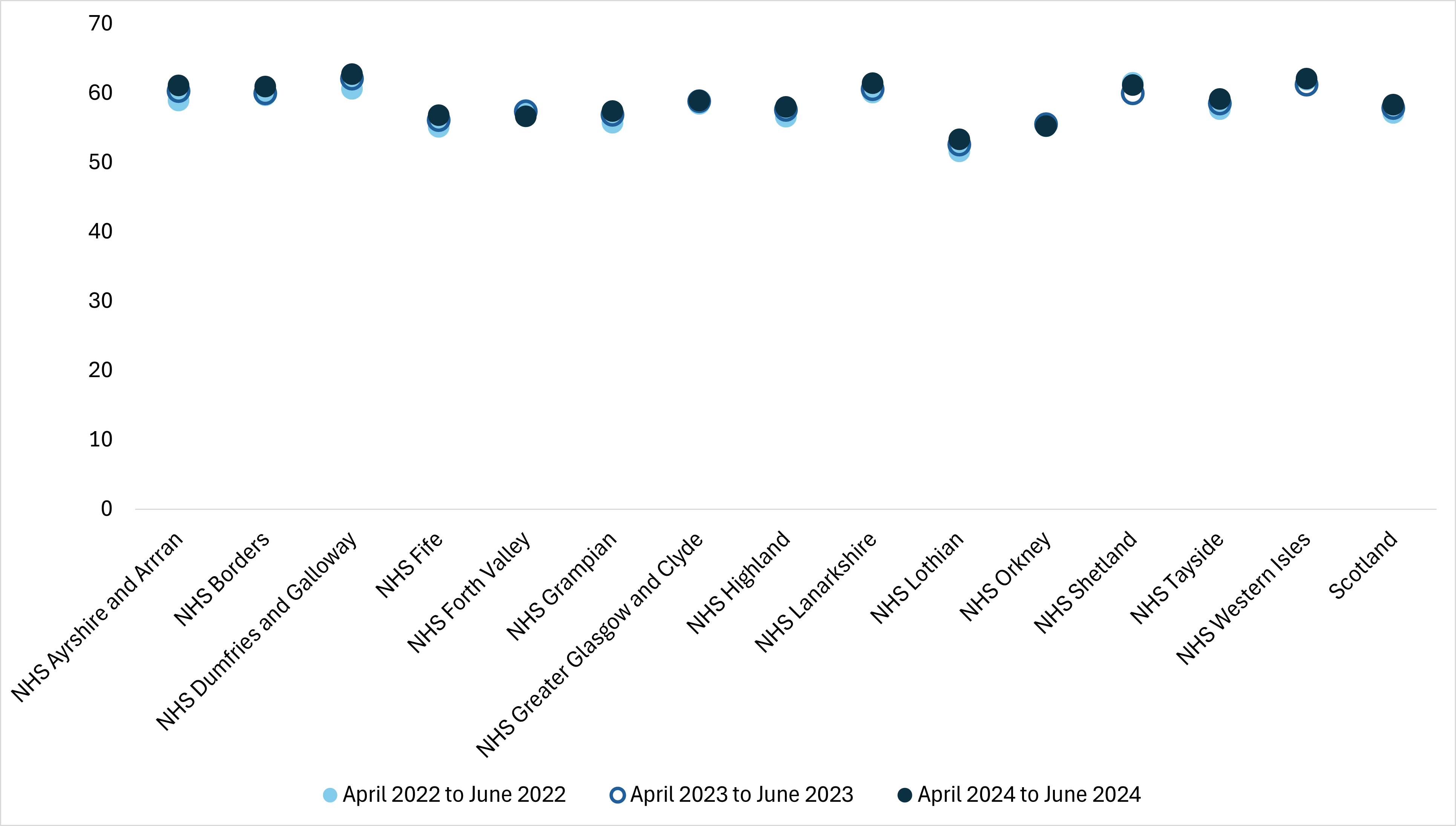
NTI: Adults (≥18 years old) prescribed long-term (≥2 years) antidepressants as a proportion of adults in receipt of antidepressant medications
Click on the chart to view a larger version.
An appropriate course of treatment for depression can be six months for the first episode of depression, or 12 or 24 months of treatment, depending on the number of depressive episodes and relapses. Long-term use is considered as more than two years of treatment and encompasses a growing number of people less likely to have their antidepressant reviewed, than those who have recently been initiated on treatment or receiving a shorter course. The longer an individual receives an antidepressant, the less frequently it, or the condition it is treating, is reviewed. For some they may be ‘lost in the system’ and inadvertently continue treatment that is no longer needed, and in others the antidepressant treatment may be ineffective or causing adverse effects.
Some prescribers may be less comfortable reviewing psychotropic medicines such as antidepressants, and may be apprehensive of reducing or stopping antidepressant therapy. This may be due to concerns about relapse or recurrence of illness, and/or antidepressant discontinuation/withdrawal symptoms, all of which may result in inappropriate long-term use where treatment is no longer required.
Reviewing people receiving the same antidepressant for two years or more can result in one in four people having a change in treatment, reduction, or stopping their antidepressants.
Actions
- Health boards and prescribers to ensure appropriate use of antidepressants, considering licensed indications and duration of therapy
- The 'What matters to you' approach should assist the individual to achieve goals which have been identified and developed in partnership with clinicians.
- Access to and availability of non-pharmacological options, including psychosocial and/or psychological interventions, should be encouraged and pursued where appropriate
- Review effectiveness, tolerability and compliance on an ongoing basis
- Any reduction/stop should be gradual to minimise discontinuation effects
- Some individuals may be more sensitive to discontinuation than others
- Review and reduce dose every one to four weeks, or as guided by the individual’s needs and/or preferences. See guidance for suggested dose reductions
- The 7-Steps review process should be used for all medication reviews.
- Individuals can be identified using the Scottish Therapeutics Utility (STU) in GP practices.
Notes:
- Age limited to 18 years and over due to licensing, however there may be some individuals under 18 years who are prescribed off-licence and should have regular follow-up by specialists. These individuals will not be identified in current STU searches.
- In NTIs, two years or more treatment is assessed as those received more than 10 prescriptions in a 24-month period of the same antidepressant medication, with medicine issued at any point in the first three months and an issue in the last three months. It does not include anyone who may have changed antidepressant during that time. This is measured against the count of people prescribed an antidepressant at the midpoint of the last three months.
- Antidepressants included are those in BNF legacy section 4.3, including tricyclic and related antidepressants, monoamine-oxidase inhibitors, SSRIs, other antidepressant drugs. Exclusions: injectables.