If you have comfort and experience with the following induction protocol, please use. However, use an induction protocol you can administer with confidence.
Trauma RSI
Aim:
- Provide strategy for RSI in major trauma patients.
- Improve safety for hypovolaemic trauma patients.
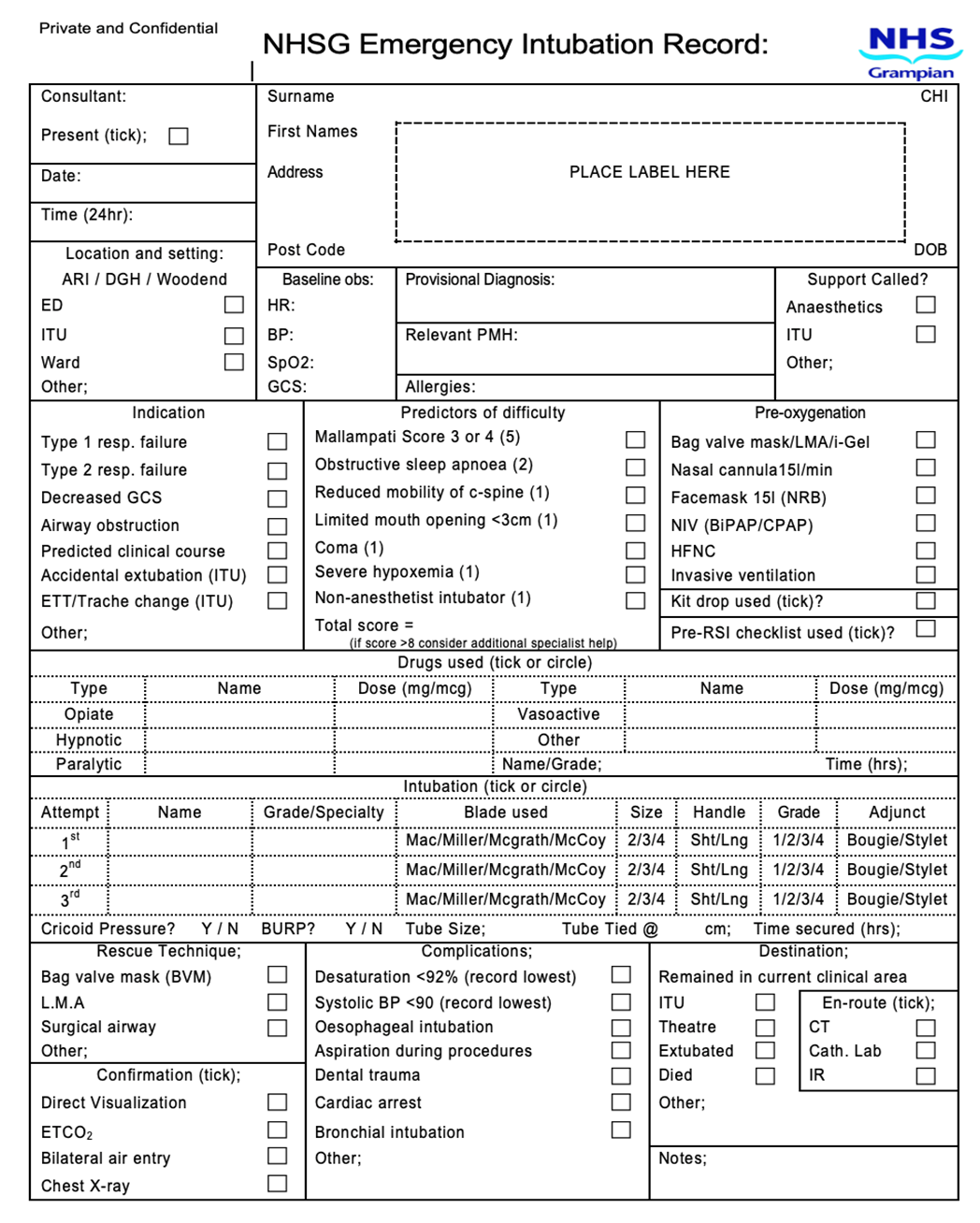
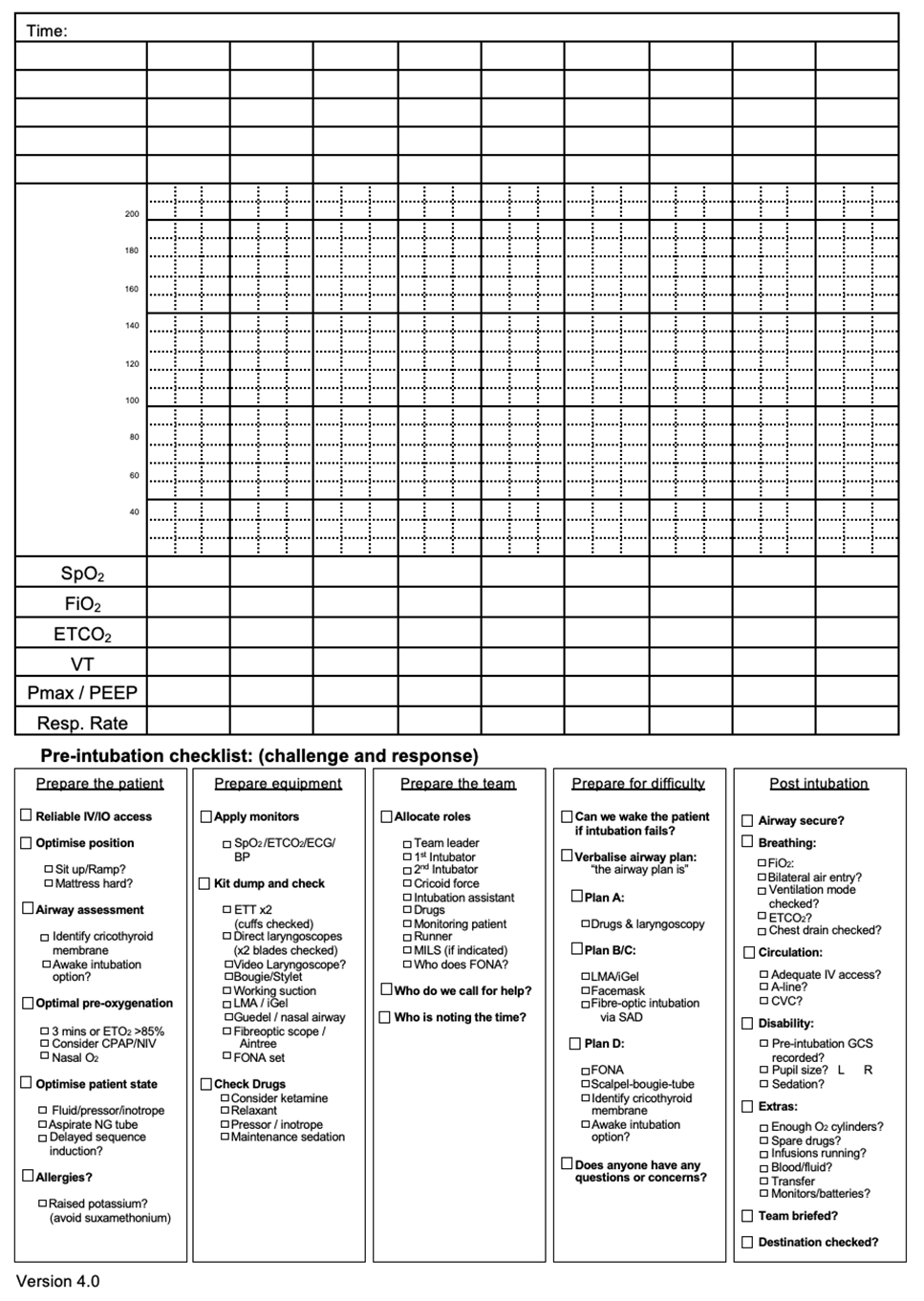
Pre-RSI phase
- Standard pre-induction preparations/checks
- Prepare ketamine 200mg/20mls. Rocuronium 100mg/10mls. Fentanyl 500mcg/10mls
- Determine degree/cause of shock + treat.
Euvolaemia (3, 2, 1)
- Fentanyl - 3mcg/kg
- Ketamine - 2mg/kg
- Rocuronium - 1mg/kg
Hypovolaemia (1, 1, 1)
- Fentanyl - 1mcg/kg
- Ketamine - 1mg/kg
- Rocuronium - 1mg/kg
Severe hypovolaemia (1, 1)
- Ketamine - 1mg/kg
- Rocuronium - 1mg/kg
Notes
This document provides a guide to assist with managing induction of anaesthesia in patients with major injury and does not attempt to cover all aspects of trauma patient Mx.
3,2,1
- This strategy is aimed at the trauma patient requiring anaesthesia without coexisting hypovolaemia e.g. combative patient with or without head injury, burns patient etc.
- Tachycardia/hypertension are not usually an issue post induction if appropriate does of opiate is used.
Post induction
- Hypertension post induction should be managed primarily with volume resuscitation plus exclusion of obstructive cause of shock e.g. tension PTX, tamponade.
- Ensure adequate anaesthesia post induction and resuscitation/restoration of systemic blood pressure.
Credit: RIE major trauma clinical guidelines

 Aberdeen Major Trauma Centre clinical guidelines (North of Scotland trauma guidelines)
Aberdeen Major Trauma Centre clinical guidelines (North of Scotland trauma guidelines)