Hearing Impairment (deafness)
 zPathways - in development
zPathways - in development

What is hearing impairment?
The term ‘deaf’ has been used throughout this resource to refer to all levels of hearing loss in children, including a partial or total loss of hearing. This includes children who may be described as having a ‘hearing loss’, ‘hearing impairment’, or ‘deaf’, and includes children who have glue ear.
What is deafness?
• Deafness occurs when one or more parts of the ear are not working effectively.
• Deafness presents in around 1 in 1000 births; however, only 50% of deaf children are born deaf. The remaining 50% may lose their hearing progressively or suddenly.
• 90% of deaf children are born to parents with little or no experience of deafness.
• Children from black and minority ethnic communities are 2-4 times more likely to experience deafness than those from other backgrounds.
Understanding deafness
The ear has two main functions.
• It receives sound and converts it into signals that the brain can understand.
• It helps us to balance.
The two functions are closely related.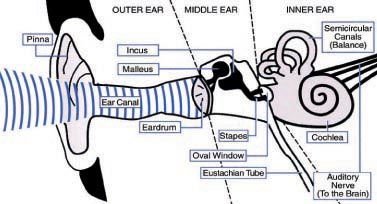
The ear is the first part of the hearing system. The pinna (the outside part of the ear) catches sound waves and directs them down the ear canal. The waves then cause the eardrum to vibrate. These vibrations are passed across the middle ear by three tiny bones: the malleus, incus and stapes (sometimes known as the hammer, anvil and stirrup, known together as the ossicles). The bones increase the strength of the vibrations before they pass through the oval window into the cochlea.
The cochlea looks like a snail’s shell. It is filled with fluid and contains thousands of tiny sound-sensitive cells. These cells are known as hair cells. The vibrations entering the cochlea cause the fluid and hair cells to move, much like the movement of seaweed on the seabed when waves pass over it.
As the hair cells move, they create a small electrical charge or signal. The auditory nerve carries these signals to the brain where they are understood as sound.
For an ear to work fully and allow us to pick up sound, all of these parts must work well.
There are two main types of deafness.
• Sensorineural deafness, or nerve deafness as it is sometimes called, is a hearing loss in the inner ear. This usually means that the cochlea in the inner ear is not working effectively. Sensorineural deafness is permanent.
• Conductive deafness means that sound cannot pass efficiently through the outer and middle ear into the inner ear. This is often caused by blockages such as wax in the outer ear, or fluid in the middle ear (glue ear). Glue ear is a very common condition, especially in pre-school children.
It is possible for children to have a combination of sensorineural and conductive deafness. This is known as mixed deafness. One example of mixed deafness is when someone has glue ear as well as permanent sensorineural deafness. It is also possible to have a permanent conductive deafness, but this is less common.
Very few deaf children have no useful hearing. Most deaf children can hear some sounds at certain frequencies and loudness, and with the use of hearing aids they are often able to hear more sounds.
Levels of deafness
The level of a child’s deafness can be described as:
• decibel (dB) hearing level, or
• ‘mild’, ‘moderate’, ‘severe’ or ‘profound’.
Below are the terms used to describe levels of deafness and the decibel hearing levels they refer to.
Level of deafness Hearing level in decibels (dB)
Mild 21-40
Moderate 41-70
Severe 71-95
Profound 95+
The words ‘mild, moderate, severe and profound’ can be misleading:
• a ‘mild’ loss is not insignificant – a child will need hearing aids to access the details of speech
• a child with ‘moderate’ loss can hear a lot of sound, especially the rise and fall of speech, but will need hearing aids to hear speech clearly
• ‘severe’ sounds bad but, with hearing aids, a child should be able to hear speech clearly
• some children with a ‘profound’ loss will benefit from hearing aids, but some may require cochlear implants to provide good levels of hearing.
In some rare cases, a child may not be able to use hearing technology. There are also families who choose not to use hearing technology with their child as a cultural choice. If a child does not have access to spoken language, they must have access to an equivalent visual language. British Sign Language (BSL) offers a full, rich and expressive language model, and is now Scotland’s fourth national language. Scottish Government’s BSL National Plan asks all national bodies, including NHS Scotland, to consider how they will promote BSL through their services.
If a family does not give a child access to a consistent language model, either through spoken language with the assistance of hearing technology, or sign language, this can be considered neglect.
Auditory Neuropathy Spectrum Disorder (ANSD) occurs when sounds are received normally by the cochlea, but become disrupted as they travel to the brain.
Children with ANSD are likely to have greater difficulty understanding speech and distinguishing one sound from another than a child with a similar level of hearing, especially in the presence of background noise. The term ‘spectrum disorder’ helps with the understanding that ANSD affects children in different ways, with symptoms ranging from very mild to very severe.
What to look out for?
• Universal Neonatal Hearing Screening Programmes (UNHSP) were introduced into Scotland in April 2005. The aim of this early screening is to diagnose children with deafness at an early age and to provide hearing amplification as soon as possible.
• In general, babies who are born deaf are now provided with hearing aids from 2 to 3 months of age.
• Research has proven that for children who are diagnosed as deaf and have no additional needs, but are provided with correct amplification and early intervention support by 6 months of age, their speech, language and communication will develop along normal lines. It is critical that the amplification is fitted appropriately, allowing auditory access to all the sounds of the native language within the first year of life, thereby increasing the probability of the development of good spoken language.
• If hearing aids do not provide adequate amplification for a child they will be referred for assessment to ascertain if cochlear implants would be appropriate. A cochlear implant is a type of implanted hearing device that converts sound into electrical signals. It is fitted during an operation.
• Children with additional needs should also have amplification provided as soon as possible in order to obtain the best outcomes. It is also imperative that functional hearing and speech, language and communication development is closely monitored as a child could have a deteriorating loss. This is related to the cause of the original hearing loss - for example children with perinatal CMV may have a slowly progressive hearing loss. Children with enlarged vestibular aqueducts may also have a progressive loss.
• Trauma and illness later in childhood can also result in a hearing loss e.g. tumour, meningitis, glue ear which can have an impact on speech, language and communication development.
There are several things to watch out for that may be indicative of a hearing loss e.g.:
• They do not respond to sounds, music or voice
• They do not react to loud sounds
• They strain to hear
• They appear very watchful
• They misunderstand things you say
• They withdraw from social situations
• They ask you to repeat things
• There is a deterioration in a child's behaviour
Please see attached questionnaires (NHS Greater Glasgow and Clyde) for further advice on monitoring level of hearing in an infant/young child and older child.
Anticipated Outcomes
For the majority of deaf children, whatever their level of hearing loss, the outlook is very positive. We generally expect children to develop normal speech and language, although there are a few contraindications which may affect outcomes:
- chronic issues with glue ear
- inconsistent hearing aid use
- poor parental support
- late diagnosis of hearing impairment
- additional support needs
How you can help: Key messages
For children already diagnosed as deaf:
A diagnosis of deaf in an infant soon after birth can be a very emotionally draining experience for parents. Health visitors can provide emotional support to parents encourage:
• Consistent hearing aid/cochlear implant use in the infant.
• A good listening environment in the home. For example spending some time with the television, radio etc off
• To link with the child's speech therapist, audiologist and teacher of the deaf.
For children with a suspected hearing loss:
• Refer the child to audiology or encourage the family to seek referral to audiology through their GP.
• Support the establishment of a good listening environment in the home. This benefits all children, not just those diagnosed as deaf.
What does a Speech and Language Therapist do?
There are Specialist Speech and Language Therapy Services for the Deaf/Hearing Impairment in many NHS Board areas in Scotland although not all. Those areas who do not have specialist provision have access to advice through the Clinical Excellence Network (CEN).
A Specialist Speech and Language Therapist for the Deaf/Hearing Impairment has normally undertaken additional training in working with deaf children and in sign language. The pattern of working varies between NHS Board areas, however in some areas speech and language therapists work with families from the point of diagnosis, whereas in other areas they become involved as needed when the child is older.
A specialist speech and language therapist can:
• help families to understand their child’s deafness and its impact
• provide support to families of children newly diagnosed with deafness in use of hearing aids/cochlear implants
• promote the use of the family’s first language (including BSL)
• provide information about various communication methods to allow the parents to make an informed choice on the preferred communication method
• encourage consistent use of hearing aids/cochlear implants during waking hours in order that children will have the best outcome in terms of speech, language and communication
• give support and advice to families to promote the best listening environment for the child
• provide families with the skills necessary to promote optimal outcomes in respect of speech, language and communication development in their child regardless of what communication method the family choose
• liaise with other professionals to share information and provide support
e.g. audiology, teachers of the deaf, health visitors, paediatricians
• provide an advisory service for non-specialist speech and language therapists working with deaf children
• provide training for non-specialist speech and language therapists and other professionals
Further reading/resources
• National Deaf children's Society (NDCS)
Available from: http://www.ndcs.org.uk/
• Universal Neonatal Hearing Screening Programmes (UNHSP) http://www.nsd.scot.nhs.uk/services/screening/UNhearingscreening/index.html
References
• Universal Neonatal Hearing Screening Programmes (UNHSP) http://www.nsd.scot.nhs.uk/services/screening/UNhearingscreening/index.html
• Yoshinaga Itano, C. & Sedey, A. (2000) Speech development of deaf and hard of hearing children in early childhood: Interrelationships with language and hearing , The Volta Review, 10092), 181-212.
• Yoshinaga Itano, C. (2000) Development of audition and speech: implications for early intervention with deaf and hard of hearing infants. The Volta Review, 10092), 213-236.
• Yoshinaga-Itano, C. (2006). Early Identification, Communication Modality, and the Development of Speech and Spoken Language Skills: Patterns and Considerations. In M. Marschark & P.E. Spencer, Advances in the spoken language of deaf and hard-of-hearing children. New York: Oxford University Press, pp. 298-327.