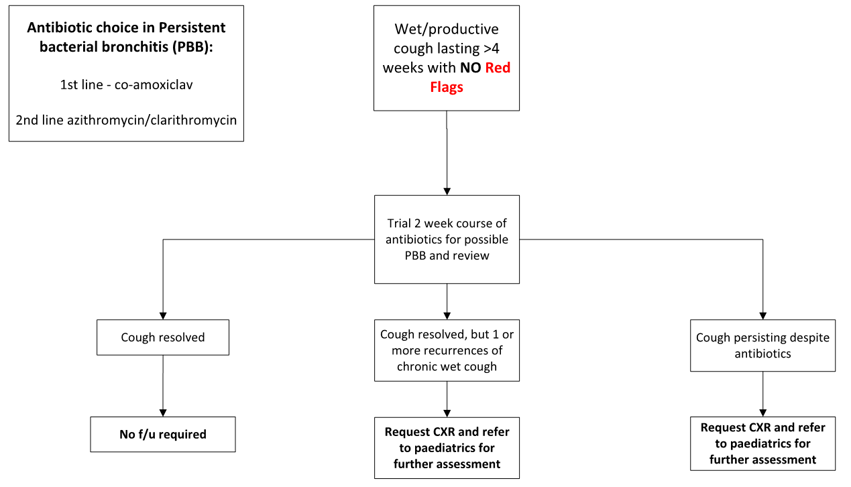
Persistent bacterial bronchitis (PBB)
- Defined as: A continuous chronic wet / productive cough (>4 weeks) without any signs / symptoms suggestive of other causes of wet / productive cough that resolves with 2 to 4 weeks antibiotics
- Almost exclusive to children between 1 to 6 years age
- Obtain sputum culture before antibiotics if possible, in older children
- A trial of 2 weeks co-amoxiclav is advised if PBB suspected
- Do not prescribe repeated courses of antibiotics for PBB, refer if concern of recurrence of PBB (can be a precursor to bronchiectasis)
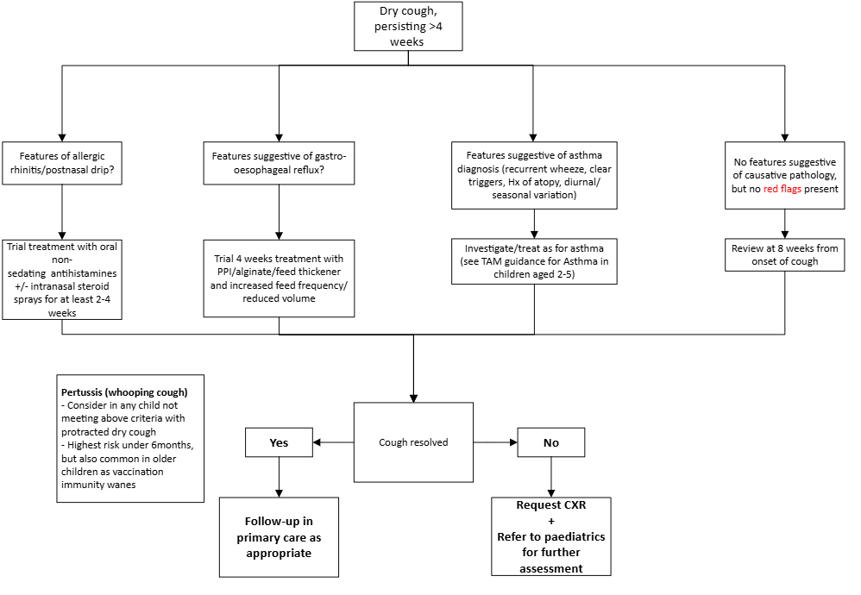
Asthma
- Cough variant asthma is rare in children; Asthma diagnosis is unlikely if there is no history of recurrent wheeze episodes
- Consider asthma if presence of potential triggers, seasonal variation, diurnal variation, family / personal history of atopy
- Refer to asthma guidelines for investigation/treatment
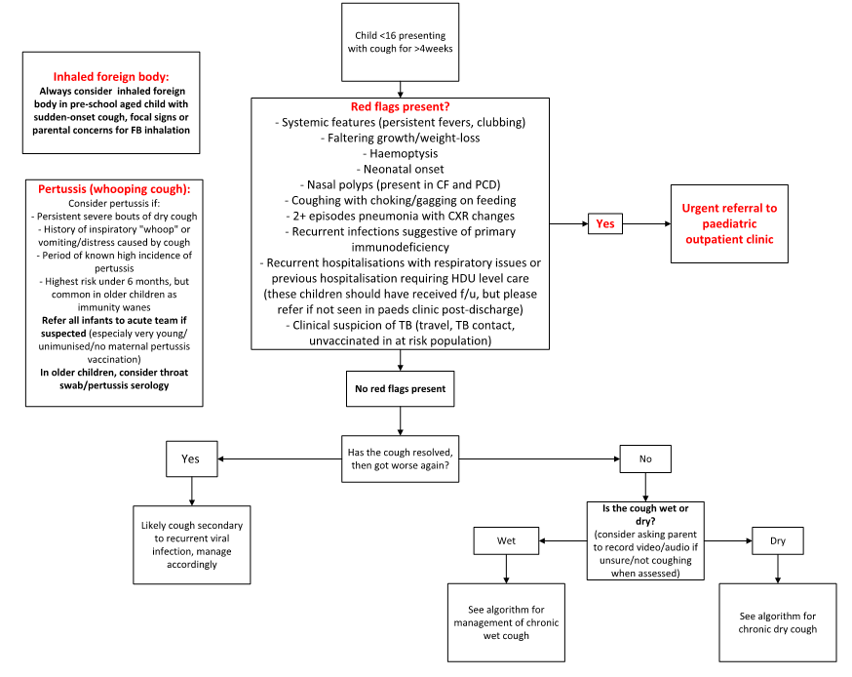
Inhaled foreign body
- A possibility in any sudden-onset cough in otherwise healthy pre-school child
- Examination may reveal persistent focal signs
Gastro-oesophageal reflux (GORD)
- Consider if there is a clinical history suggestive of reflux
- Do not routinely offer anti-acid therapy for chronic cough with no other features of GORD
Postnasal drip
- Often presents with family/personal history of atopy and persistent nasal congestion
- Consider trial of antihistamine therapy if suspected as cause for chronic cough
- Intranasal steroids and saline drops can also be useful
Sinister pathologies
- Eg Cystic fibrosis, TB, immune deficiency syndromes, etc. May present in a wide variety of manners
- Refer if there is a clinical concern
Habit cough (somatic cough syndrome)
- A diagnosis of exclusion
- Typically presents as a cough with a high degree of variability, distractibility
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland