North of Scotland major trauma guidelines
North of Scotland major trauma guidelines


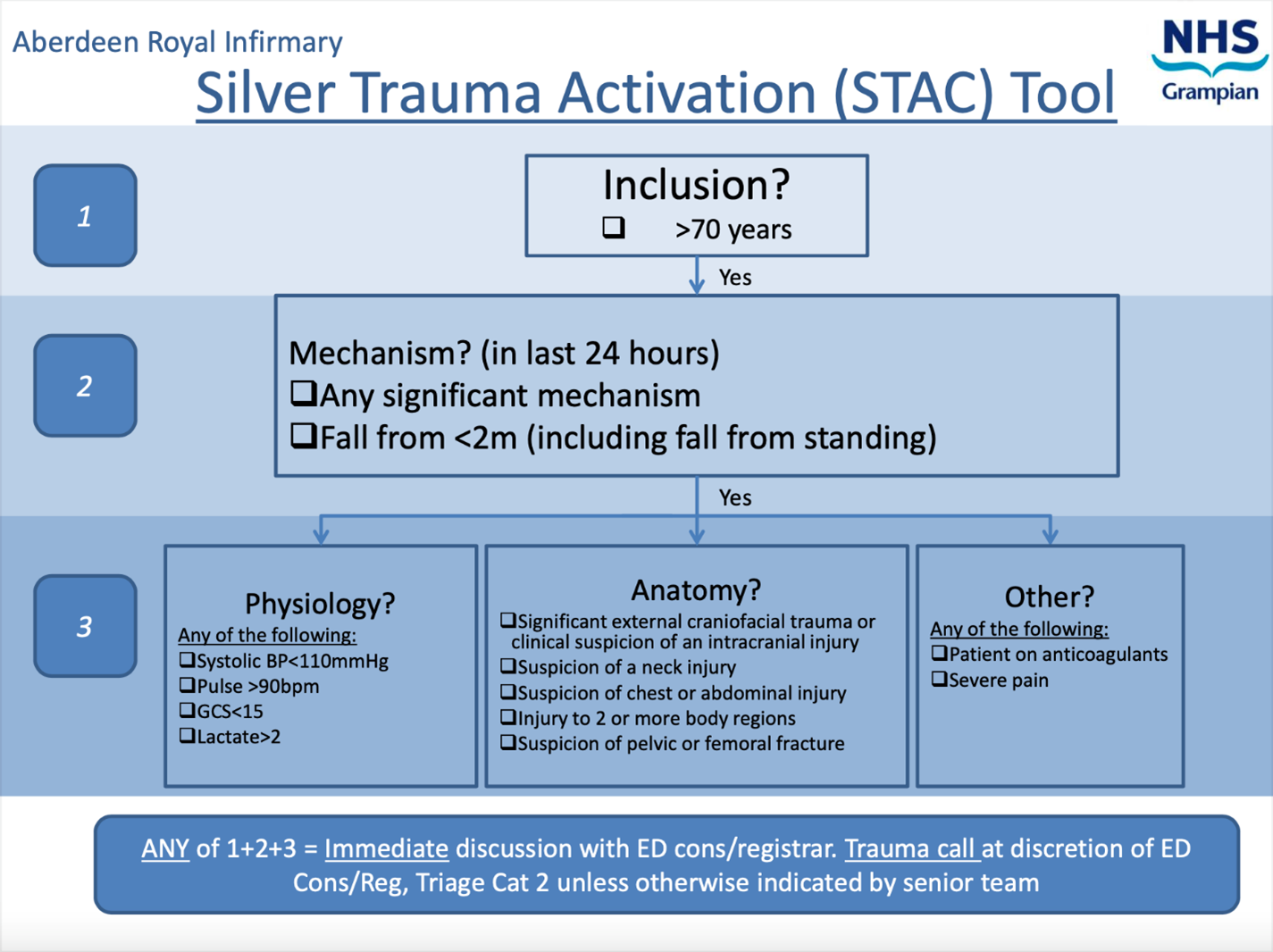
- Elderly patients should receive the same trauma care following admission to that given to younger patients.
- Advanced age is not an absolute predictor of poor outcomes following trauma and should not be used as the sole criterion for denying or limiting care.
- An initial aggressive approach should be pursued for management of the elderly patient unless in the judgement of an experienced consultant the injury burden is severe, and the patient appears moribund.