Severe Head Injury
These will be patients with significant risk factors described in Category 1 or Category 2 and may have a reduced GCS and will usually be managed in resus.
Consider the need for a Trauma Call if not already triggered.
Perform a primary survey and ensure the child’s airway, cervical spine, breathing and circulation are secure.
Prevent secondary brain injury by maintaining adequate ventilation and oxygenation.
Control any seizures.
Always consider the need for appropriate analgesia .
In conjunction with ED Consultant /PICU/ Neurosurgery consider measures to decrease intracranial pressure:
- Nurse 300 head up after correction of any shock
- Maintain adequate BP
- Aim to ventilate to a normal pCO2
- Consider IV 3% NaCl 3ml/kg as a bolus or IV Mannitol over 20minutes
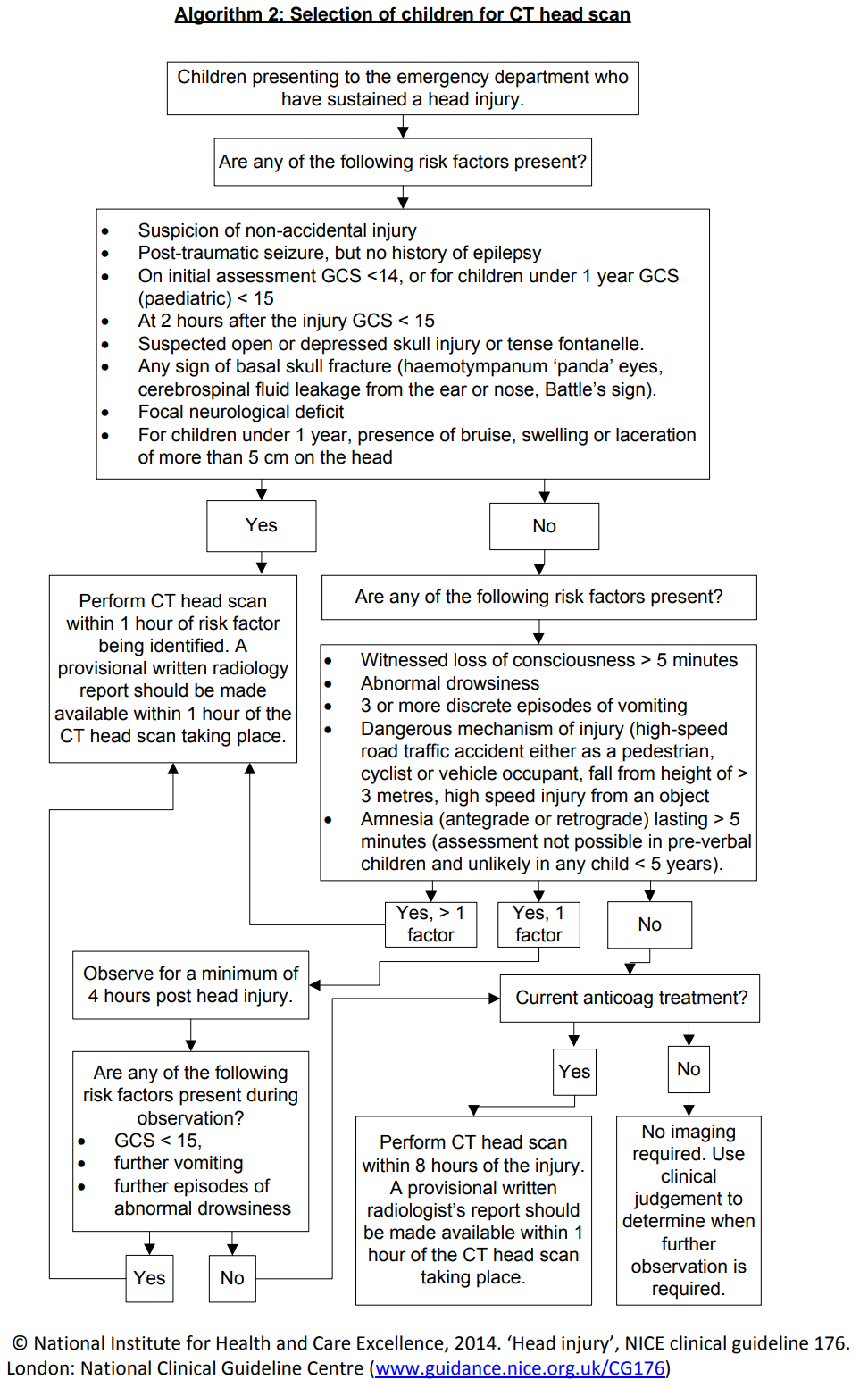
Arrange an immediate CT head scan to be performed within 1 hour.
Moderate Head Injury
These patients will have some of the significant risk factors described in Category 2 or Category 3 but will not have a reduced GCS and will usually be managed in Majors.
Always consider the need for appropriate analgesia.
These children require 30 minutely neurological observations (GCS, pupils and limb power, HR, RR, BP) documented on a PEWS chart whilst in ED.
Senior advice should always be sought regarding the need for a CT head scan.
If these patients do not fulfil the criteria for a CT head scan then they should be observed in ED for a minimum of 4 hours from the time of injury before they can be discharged (see Discharge from ED section below).
These patients should be able to tolerate oral fluids in ED and be steady on their feet before discharge.
There is no clear evidence for or against the use of Ondansetron. Whilst there is no definite increase in missed pathology, there is a slight increase in the re-attendance rate in head injury patients who have had Ondansetron.
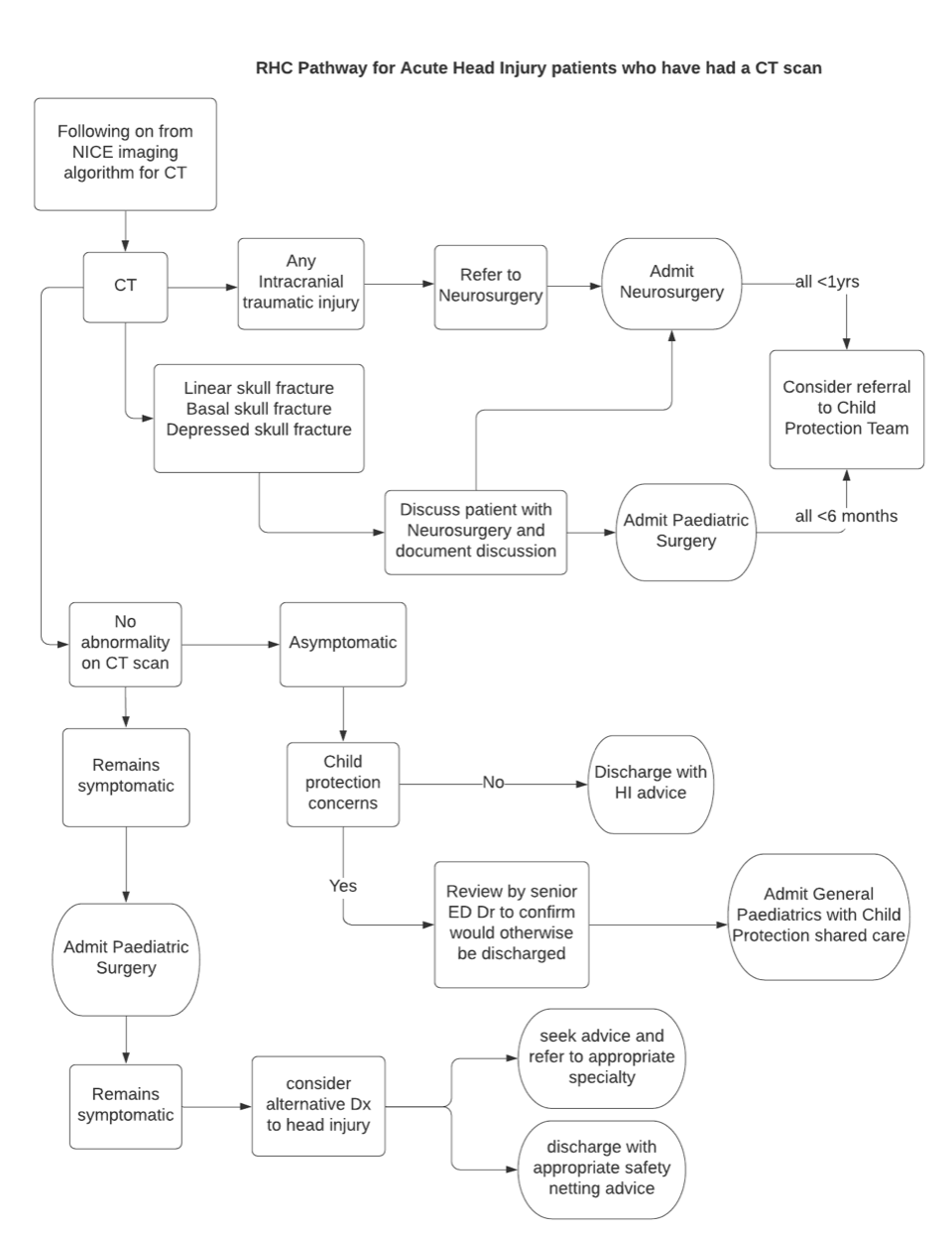
Patients who have had a CT head scan should continue to be monitored and discussed appropriately as per the Pathway for Acute Head Injury Patients who have had a CT scan (see section below)
Patients who had a dangerous mechanism of injury and other injuries in addition to their head Injury, should be referred to the Paediatric Surgical team for review and possible admission.
Mild Head Injury
Any patient with significant co-morbidities (including CSF drainage devices-“shunts”) should be discussed with the ED Consultant.
Any patient on anticoagulants or with an underlying coagulation or haematological disorder should be discussed with the ED Consultant.
Always consider the need for appropriate analgesia.